
Wentworth Institute of Technology. O. Shakyor, MD: "Buy cheap Depakote - Proven Depakote online OTC".
Two patients’ sta- shows a large syrinx (*) in the cervical spinal cord depakote 250mg visa medications that cause hyponatremia, which tus post T-tube insertion for cervical spine syringomyelia was successfully decompressed following T-tube inser- decompression purchase 250 mg depakote with amex medications causing gout. Reported complications include malfunction 500mg depakote sale treatment resistant anxiety, an intrathecal catheter and tunneling a distal catheter malposition order depakote 500 mg on-line symptoms diverticulitis, hemorrhage, and infection. The patient has a his- position with gravity-actuated valve component (encir- tory of pseudotumor cerebri and cerebrospinal fuid rhi- cled), which is magnifed in the inset norrhea. Frontal radiograph shows the lumboperitoneal shunt catheter in position with a pro- grammable valve component (encircled), which is magni- fed in the inset 6 Imaging of Cerebrospinal Fluid Shunts, Drains, and Diversion Techniques 277 6. In particular, the sagittal phase- Endoscopic fenestration of the anterior foor of contrast cine sequence is the gold standard for the third ventricle (Liliequist’s membrane) cre- evaluating cerebrospinal fuid fow dynamics. This procedure bypasses obstruction at across the foor of the third ventricle is charac- the level of the Sylvian aqueduct and restores teristic. A jet of cerebrospinal fuid can also cerebrospinal fuid fow out of the ventricular manifest on T2-weighted sequences. Third ventriculocisternostomy is a resolution heavily T2-weighted cisternogram- minimally invasive alternative to shunt implan- type sequences, the normal Liliequist’s tation and is indicated for patients with aque- membrane can be identifed. Following third ductal stenosis, obstructive tumors, and ventriculostomy, the membrane will appear obstructive cysts. Rarely, tumor cysts are decom- procedure consists of creating a burr hole, intro- pressed into the ventricular system as a last resort ducing a cannula and endoscope into the lateral (Fig. This approach is generally avoided ventricles, and coagulating the septum pellu- due to the risk of subsequent hydrocephalus sec- cidum to allow communication between the right ondary to malabsorption from the cyst contents. Postoperative T2-weighted 6 Imaging of Cerebrospinal Fluid Shunts, Drains, and Diversion Techniques 279 6. Balloon dilatation can be performed to expand the obstructed aqueduct of Sylvius (Fig. Alternatively, a small-caliber fexible endoscope can be used to create a perforation in the offend- ing membrane and to introduce a stent. Following aqueductoplasty, the third and lateral ventricles usually decrease in size. Nevertheless, choroid plexus cauteriza- tion is often performed in conjunction with 6. Choroid plexus surgery is an option for treat- Choroid plexus papillomas can cause hydro- ing hydrocephalus in patients with suspected cephalus due to overproduction of cerebrospinal cerebrospinal fuid overproduction and patients fuid with rates of over 1. Total surgical resec- cauterization can be performed endoscopically tion of the tumor and vascular pedicle is the treat- and consists of coagulating a portion of the ment of choice. After resection, the hydro- treated choroid plexus can be appreciated cephalus usually resolves (Fig. Interestingly, following choroid treatment for hydrocephalus after resection may plexus cauterization alone, ventricular size be required due to intraventricular hemorrhage, does not necessarily decrease signifcantly, infammation from surgery, and mechanical dis- although sulci become more prominent tortion of the ventricular system. Sequelae of left ventricular fenestra- ventricles, particularly the atrium of the left lateral ven- tion are also demonstrated, with resultant decompression tricle, resulting in cranial vault deformity. The etiology for the signal changes is Catheterization likely attributable to compression of the corpus callosum against the rigid falx cerebri from 6. These changes Due to its proximity to lateral ventricle shunt tra- are typically not associated with symptoms and jectories, the corpus callosum is prone to injury should not be misinterpreted as neoplasm, white during catheter insertion. This can result in linear matter disease, or leukoencephalopathy in par- areas of high T2 signal in the corpus callosum ticular, the corpus callosum can acquire a scal- adjacent to the catheter. Corpus callosal swelling loping deformity, which is best appreciated on can also occur after ventricular shunting for long- sagittal images. The Intracranial hemorrhage may present soon after calcifcations tend to occur at the margins of the ventricular catheterization or it can be delayed. When bilateral, these have chymal friability, venous occlusion, coagulopa- been termed “armored brain. The Valve Setting Alteration accumulation of cerebrospinal fuid can lead to ventricular enlargement, unless there is extensive 6. Enlargement of the temporal indwelling ventricular shunts is a sign of shunt horns is among the earliest fndings of this com- failure. Other signs include effacement of the alter the pressure setting of most percutaneous sulci and transependymal fow of cerebrospinal programmable cerebrospinal fuid shunts and fuid. Hydrocephalus can result in sutural diasta- may also result in acute hydrocephalus, mimick- sis and enlargement of cranial diameter in ing shunt malfunction, if the setting is not children. On imaging, disparate sizes of the ventri- cles are apparent, and contrast does not enter 6. The compartmentalized collection obstruction is often at the foramen of Monro, but of cerebrospinal fuid can lead to symptoms of can occur anywhere in the ventricular system. Isolated ventricles that are eate the presence of loculations by the lack of not enlarging can be diffcult to differentiate from communication of the contrast material with the asymmetric ventricles, which may also be rest of the ventricular system (Fig. Midline shift and progressive increase uncommon phenomenon that can occur in the in size of the ventricle suggest trapping over sim- setting of ventricular shunting with adhesion for- ple asymmetry of the ventricles. If there is any mation and represents a form of focal hydroceph- doubt, short interval imaging follow-up can be alus. This process may may result from reduced brain compliance, often extend into the cervical spine and rarely results in due to the use of a siphoning-valve shunting cervical myelopathy. However, elderly patients are appear to be very small and do not increase in usually asymptomatic due to brain atrophy. The condition can be very seri- children may also lead to hyperostosis cranii ex ous and should not be misinterpreted as small vacuo. The most image both ends of the shunt system in sus- common causative organisms are pected cases of infection. On shunt-associated infections mainly include ven- imaging, ventriculitis can manifest as periven- triculitis (ependymitis) and meningitis. Treatment generally consists of associated infection ranges from 2% to 40% per removal of the entire shunt device, an interim shunting procedure. Distal shunt-associated period of external ventricular drainage and anti- infections include cellulitis and subcutaneous biotic therapy, and eventual replacement of the and intra-abdominal abscesses, which can be shunting device at a different site. There are also bilateral cererbral diffusion in the occipital horns of the bilateral lateral convexity subdural fuid collections, left larger than right ventricles. The tip of the catheter exits the skin of enhancing fuid collections along the prior shunt tract. Retraction into the abdominal wall can lead ventricles can be challenging particularly in to the formation of a pseudocyst within the sub- patients with small ventricles. Migration of the that suboptimal ventriculoperitoneal shunt posi- distal shunt into the rectum must be preceded by tioning occurs in about 25% of cases and that in bowel perforation. Catheter malposition can migrated shunt device components and associ- compromise cerebrospinal fuid drainage and ated complications. Management may include lead to injury of brain parenchyma and associated laparotomy with catheter removal and replace- symptomatology (Fig.
Syndromes
- Counting carbohydrates
- Accidents or injuries to the surface of the eye (such as chemical burns or sports injuries)
- Loss of ability to interact with others
- Have a vocabulary that is below the level of other children the same age
- The person loses consciousness at any time.
- If the pain is high up in your abdomen and occurs after meals, antacids may help, especially if you feel heartburn or indigestion. Avoid citrus, high-fat foods, fried or greasy foods, tomato products, caffeine, alcohol, and carbonated beverages.
- Open pleural biopsy
Rapid osmotic diuresis in elderly patients metabolic insults (cytotoxic edema) order depakote 250 mg without prescription medications ending in zine, such as hypox- can also occasionally cause a subdural hematoma emia or ischemia generic depakote 250mg fast delivery symptoms strep throat, results from failure of brain cells due to rupture of fragile bridging veins entering the to actively extrude sodium causing progressive cel- sagittal sinus depakote 250mg discount medications similar to vyvanse. The neurological examination should docu- having a lesser maximal efect than mannitol and ment mental status and any sensory or motor requiring up to 30 min cheap depakote 500 mg online medicine 44390, may have the additional defcits. Laboratory evaluation should be synergistic, but requires close monitoring of the rule out corticosteroid-induced hyperglycemia, serum potassium concentration. Anticonvul- sant blood concentrations may be measured, Anesthesia & Craniotomy for particularly when seizures are not well controlled. Patients with Mass Lesions Premedication Intracranial masses may be congenital, neoplastic Sedative or opioid premedication is best avoided if (benign or malignant), infectious (abscess or cyst), intracranial hypertension is suspected. Craniotomy is commonly undertaken for neo- Corticosteroids and anticonvulsant therapy should plasms of the brain. Slowly growing masses are frequently asymp- pressure monitoring and bladder catheterization tomatic for long periods (despite relatively large size), are used for most patients undergoing craniotomy. Common presenta- procedures, positioning, and surgical manipulation tions include headache, seizures, a general decline are best managed with guidance from continuous in cognitive or specifc neurological functions, and invasive monitoring of blood pressure. Symptoms typical to arterial blood gas analyses are necessary to closely supratentorial masses include seizures, hemiplegia, regulate Pa co. Use of the The preoperative evaluation for patients undergoing internal jugular vein for access is theoretically prob- craniotomy should attempt to establish the presence lematic because of concern that the catheter might or absence of intracranial hypertension. An intravenous opioid given of the use of diuretics, the long duration of most with propofol blunts the sympathetic response, par- neurosurgical procedures, and its utility in guid- ticularly in young patients. Neuromuscular function should kg, is efective in preventing tachycardia associated be monitored on the unafected side in patients with intubation in lightly anesthetized patients. Additional monitors for attempted prior to the establishment of deep anes- surgery in the posterior fossa are described below. The head may also be turned to the side rial blood pressure can be equally detrimental by to facilitate exposure. Cooperative patients nized disconnections may be increased because the can be asked to hyperventilate during preoxygen- patient’s airway will not be easily assessed afer surgi- ation. All patients receive controlled ventilation once cal draping; moreover, the operating table is usually the propofol has been injected. Patients who will remain intubated should be sedated to prevent Anesthesia can be maintained with inhalation agitation. Extubation in the operating room requires anesthesia, total intravenous anesthesia techniques special handling during emergence. Even though periods of stimulation the skin is being closed, the patient should resume are few, neuromuscular blockade is recommended— breathing spontaneously. Should the patient’s head unless neurophysiological monitoring contradicts be secured in a Mayfeld pin apparatus, care must its use—to prevent straining, bucking, or movement. Afer the head dressing is applied and intubation, skin incision, dural opening, periosteal full access to the patient is regained (the table is manipulations, including Mayfed pin placement turned back to its original position as at induc- and closure. Likewise, the α -agonist2 dexme- Rapid awakening facilitates immediate neurological detomidine can be employed during both asleep and assessment and can generally be expected follow- awake craniotomies to similar efect. Delayed awakening Hyperventilation should be continued intraop- may be seen following opioid or sedative overdose, eratively to maintain Paco2 at roughly 30–35 mm when the end-tidal concentration of the volatile Hg. Immediate should be avoided because of a potentially adverse reexploration may be required. Intravenous fuid replacement should be limited Anesthesia for Surgery to glucose-free isotonic crystalloid or colloid solu- in the Posterior Fossa tions. Hyperglycemia is common in neurosurgical patients (corticosteroid efect) and has been impli- Craniotomy for a mass in the posterior fossa pres- cated in increasing ischemic brain injury. Colloid ents a unique set of potential problems: obstructive solutions can be used to restore intravascular vol- hydrocephalus, possible injury to vital brainstem ume defcits, whereas isotonic crystalloid solu- centers, pneumocephalus, and, with unusual posi- tions are used for maintenance fuid requirements. Brain Stem Injury Operations in the posterior fossa can injure 3 vital circulatory and respiratory brainstem centers and cranial nerves or their nuclei. Such inju- ries may occur as a result of direct surgical trauma or ischemia from retraction or other interruptions of the blood supply. Damage to respiratory centers is said to nearly always produce circulatory changes; therefore, abrupt changes in blood pressure, heart rate, or cardiac rhythm should alert the anesthesiolo- gist to the possibility of such an injury. Historically, some clinicians have employed spontaneous ventilation obstruction), and, rarely, quadriplegia (due to com- during these procedures as an additional monitor of pression of the cervical spinal cord). At completion of the surgery, brain- vical spinal stenosis probably predisposes patients to stem injuries may present as an abnormal respiratory the latter injury. Monitoring brainstem audi- tory evoked potentials may be useful in preventing Pneumocephalus eighth nerve damage during resections of acoustic The sitting position increases the likelihood of pneu- neuromas. Expansion of a pneumocephalus following dural closure can com- Although most explorations of the posterior fossa press the brain. Postoperative pneumocephalus can can be performed with the patient in either a modi- cause delayed awakening and continued impairment fed lateral or prone position, the sitting position of neurological function. The head is fxed in a three-point Venous Air Embolism holder with the neck fexed; the arms remain at the Venous air embolism can occur when the 4 sides with the hands resting on the lap. Pressure points, such as the elbows, (and during any procedure) whenever the wound is ischial spines, heels, and forehead, must be pro- above the level of the heart. Entry into large cerebral venous sinuses pressure gradient can develop at some time dur- increases the risk. Central Venous Catheterization cardiac shunt (eg, patent foramen ovale [10% to 25% A properly positioned central venous catheter can incidence]). The latter are important because they can be used to aspirate entrained air, but there is only facilitate passage of air into the arterial circulation limited evidence that this infuences outcomes afer (paradoxical air embolism). Some clinicians have consid- bubbles entering the venous system ordinarily lodge ered right atrial catheterization mandatory for sit- in the pulmonary circulation, where they are eventu- ting craniotomies, but this is a minority viewpoint. Small quantities of embolized air are Optimal recovery of air following venous air 5 well tolerated by most patients. When the amount embolism is provided by a multiorifced cath- entrained exceeds the rate of pulmonary clear- eter positioned at the junction between the right ance, pulmonary artery pressure rises progressively. Confrmation of Eventually, cardiac output decreases in response to correct catheter positioning can be accomplished increases in right ventricular aferload. Intra- venous air embolism; relatively small amounts of air vascular electrocardiography is accomplished by may produce marked hemodynamic changes. Correct oxide, by difusing into the bubbles and increasing high atrial position is indicated by the appearance of their volume, can markedly accentuate the efects a biphasic P wave. The dose into the heart, the P wave changes from a biphasic to for lethal venous air embolism in animals receiving a undirectional defection. A right ventricular or nitrous oxide anesthesia is one-third to one-half that pulmonary artery waveform may also be observed of control animals not receiving nitrous oxide. Monitoring for Venous Air Embolism 2 arterial oxygen saturation might be noticed prior The most sensitive monitors available should be used. Arterial blood gas val- Detecting even small amounts of venous air embo- ues may show only slight increases in Paco as a lism is important because it allows surgical control 2 result of increased pulmonary dead space (areas of the entry site before additional air is entrained. Doppler methods employ a probe over the or coronary occlusion, which may be apparent right atrium (usually to the right of the sternum and only postoperatively. Interruption of more likely to occur in patients with right-to-lef the regular swishing of the Doppler signal by spo- intracardiac shunts, particularly when the nor- radic roaring sounds indicates venous air embolism.
Syndromes
- Antifungal drugs for yeast infections
- Arm or leg pain?
- Vegetables: 1 cup of raw vegetables, or 1/2 cup cooked vegetables, or 3/4 cup of vegetable juice
- Incest - resources
- Dry mouth.
- American Chronic Pain Association - www.theacpa.org
- Mental changes
- Cap the container. Label the container with your name, the date, the time of completion, and return it as instructed. Keep it in the refrigerator or a cool place until you return it to the laboratory.
- Treatment with steroid medicines that causes the body to retain salt
- Problems seeing shapes against a background or the difference between shades of colors
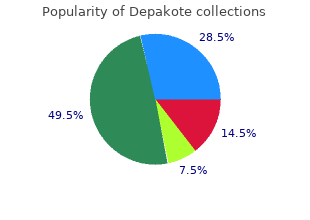
Insulin pens 250 mg depakote sale symptoms night sweats, as a means of subcutaneous insulin injection buy 500 mg depakote overnight delivery medicine ball, are an important breakthrough in insulin therapy purchase depakote 500mg symptoms 9dpiui. They constitute a more practical and easier way of insulin transport and administration com- pared to the conventional syringes generic 250mg depakote free shipping medicine upset stomach, and they achieve more precision in the administered dose. Their use is relatively simple, especially those that are only used once (prefilled pens-syringes). The pens should not be given to patients without sufficient training, and it should be ascertained that their opera- tion has been completely understood. The probability of its appearance is increased with a more intensified form of treatment (see Chapter 5). This can be due to better glycaemic control (and the consequent reduction of glucosuria), and to the appearance of hypoglycaemias (even light ones) that lead to an increase of caloric intake. Allergic reactions following the administration of human type insulin are infrequent. They are separated into local (more frequent) and systematic (more infrequent) reactions. Treatment with human insulin can cause the creation of small con- centrations of antibodies against insulin. These create problems in the activity of the hormone only when they circulate in high concentrations in the blood, which is exceptionally infrequently. Treatment of diabetes with insulin 377 The phenomenon of lipodystrophy used to constitute a non-infrequent problem in the past. Today, however, this is practically non-existent because of cleanliness and the type of insulin (human). The answer to this question is very difficult because treatment with insulin is individualized. How are the types of insulin therapy that imitate the physiologic secretion of insulin planned? The first concerns the basic secretion of insulin, which occurs continually all day and is almost constant, with the exception of two peaks, one a little before waking in the morning and the second in the afternoon hours. The second component concerns the insulin that is secreted every time that the individual receives food (Figure 28. Secretion of insulin in a normal subject during a 24-hour period 378 Diabetes in Clinical Practice quantity of ‘prandial’ insulin that is secreted depends mainly on the carbohydrate content of the meal. In order for the treatment to imitate the physiologic secretion of insulin, it is clear that both of the above components should be taken into consideration. Therefore, two types of insulin are required; one type that imitates the basal insulin secretion and a second type, with every meal, that imitates the ‘prandial’ insulin. Thus, the so-called intensified basal- prandial insulin therapy regimens were created (basal-bolus regimens). Reviewing what was previously mentioned regarding the types of insulin products, we can conclude that for the imitation of basal insulin secretion, intermediate and slow-acting insulins are to be used (in one or two injections daily), whereas before meals the rapid- and very rapid-acting insulins are to be used (an injection before each meal). Thus, various combinations result, each one of which constitutes a therapeutic regimen. The main advantage is better glucose control which leads to a reduction of diabetic complications. In the same study it was shown that intensive insulin therapy with the administration of basal- bolus insulin leads to better glycaemic control. Apart from better control, the intensive basal-bolus insulin regimens give diabetics more comfort of movement, since they acquire more free- dom as regards the schedule and content of their meals. Diabetics can have a meal whenever they want and in any quantity they want, on condi- tion of course that they inject some insulin before the meal. The dose of insulin is adapted depending on the content of the meal in carbohydrates. Treatment of diabetes with insulin 379 Other disadvantages are relative complexity, bigger weight gain, more frequent incidence of hypoglycaemia unawareness and higher financial cost. Provided there is an indication for their administration, the basic condi- tion is the acceptance of the regimen by the patient, after of course his or her thorough and objective briefing with regard to the necessity, func- tionality and precise way of application. The details of the treatment should be analysed and it should be emphasized that, together with the multiple injections, it is absolutely essential that the patient regularly monitors (at least four times a day) the glucose levels in the capillary blood. Acceptance by the patient assumes that a powerful incentive exists to achieve the best blood sugar control. This motivation is based on correct briefing and on factors such as age, maturity, educational level and psychological situation of the individual. The substitution of basal insulin secretion is achieved by administering one or two insulin injections of intermediate or slow duration of action daily. The reason for this particular time lies in the avoidance of night- time hypoglycaemia (if the injection is given earlier, the peak of action will coincide with the first morning hours of high insulin sensitivity, when the risk of hypoglycaemia is increased). The pre-bedtime injec- tion aims at placing the peak of action near the waking time, when higher needs of insulin usually exist (a period of low insulin sensitivity because of counter-regulatory hormones secretion). If only one injec- tion of isophane insulin is administered, there is often a lack of basal insulin after the noon of the following day (because of its relatively short duration of action, see Table 28. Large part the lack of basal insulin for a interval of the day is covered by the relatively prolonged action of the repeatedly injected regular insulin. In Treatment of diabetes with insulin 381 this case it is preferable to use a very rapid-acting insulin analogue (Lispro or Aspart) as ‘prandial’ insulin, so that the overlap between the insulins is decreased. This insulin has a wide peak (12–16 hours after the injection) and increased variability (in the same patient as well as among different patients) in its action profile. Theoretically, it was constructed to cover the basal secretion administered once a day. However, the increased variability in its absorption often leads to unanticipated hyper- and hypoglycaemias. Glargine is the first insulin analogue of slow action to be used in clinical practice. It differs at the molecular level compared to human insulin both in chain A as well as in chain B (Table 28. Glargine is soluble in the slightly acidic environment of the solution in which it is supplied. After its injection in the subcuta- neous tissue it is absorbed at a slow and constant rate. Its duration of action after subcutaneous injection is almost 24 hours (22 Æ 4 hours) and, in contrast to the other slow-acting insulins, it does not have a peak. Moreover, it was found that its serum levels present smaller variability in the same and/or in different patients compared to isophane insulin. These characteristics allow the substitution of the basal secretion of insulin in the forms of basal-bolus treatment to be achieved. Thanks to its long action, the insulin Glargine can be administered only once a day, either after rising in the morning or before bedtime (Figure 28.