
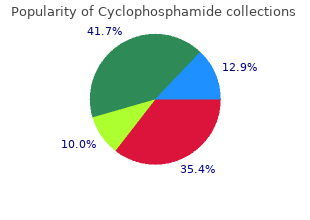
Trevecca Nazarene University. D. Shawn, MD: "Order online Cyclophosphamide cheap - Trusted Cyclophosphamide online OTC".
There are multiple other early reports of spongiform myocardium and abnormal myocardium with sinusoids generic 50mg cyclophosphamide with mastercard medications similar to cymbalta, mostly based on pathology specimens (14 generic 50mg cyclophosphamide otc art of medicine,15 cheap 50 mg cyclophosphamide with visa treatment concussion,16 buy discount cyclophosphamide 50 mg treatment centers near me,17,18,19,20,21). Adult studies have estimated its prevalence from 4 to 26 per 10,000 of the population (22,23). Before reviewing normal early myocardial development one must recognize the increase of new and eye opening data challenging traditional concepts. Young competitors represent a clear example of having increased trabeculations arising as a result of myocardial remodeling (26) (Figs. New de novo appearance of trabeculations which also is observed in pregnancy (27) could be an adaptive mechanism to increased loading conditions. Increased left ventricular trabeculation in highly trained athletes: do we need more stringent criteria for the diagnosis of left ventricular non-compaction in athletes? Reversible de novo left ventricular trabeculations in pregnant women: implications for the diagnosis of left ventricular noncompaction in low-risk populations. A specific sequence of morphogenetic steps occur in development of the normal ventricular myocardium (30). An early tubular heart is formed from the lateral mesoderm composed of three layers, one layer of myocardium, an endocardium, and a layer of cardiac jelly or extracellular matrix partitioning the two. During the second stage, the myocardium thickens, endocardial cells invaginate, and myocardial cells along the inner wall form sheet protrusions into the lumen resulting in a trabecular myocardium. It has been proposed that the trabeculations allow nutrient and oxygen exchange within the myocardium and also augment heart muscle force generation in the developing embryo (31). Stage four is progression to a spiral multilayered mature myocardium during late fetal stage (32). These characteristic myocyte arrangements are deemed important for the normal contractile process. Multiple growth factors and signaling pathways in the endocardium are deemed important in this sequential process of hypertrabeculation, compaction, and maturation of the myocardium. P57kip2 is a cyclin-dependent kinase inhibitor of the p21 family, unique to the myocardium and its trabeculae and is believed to be crucial to suppression of trabeculation (34). Other growth factors include neuregulin 1 which is produced in endocardial cells and is mediated through myocardial receptors Erb2 and 4 (35). A study in zebrafish recently demonstrated that neuregulin 1 also regulates cardiac myocyte delamination to start trabeculation as well as promoting cell proliferation (36). It has also become clear that the correct expression and amount of cardiac jelly, regulated by chromatin-remodeling factor Brg1 is required for normal development of the myocardium (39). The epicardium also produces several mitogenic factors important in myocyte development. There is interaction between epicardial, myocardial, and endocardial signaling in the regulation of myocyte maturation. Notch1-activated protein is found in the endocardial cells at the base of trabeculae (52). Thus notch signaling appears to be a critical factor in normal trabecular/compaction development. Two existing possible embryologic morphogenesis hypotheses have been proposed by Arbustini (26). These primarily involve the sarcomere proteins, typically associated with cardiac contractility, rather than crucial stages of embryologic development between trabeculation and compaction. Interestingly Mib1, regulates Notch1 ligands Jagged and Delta, once again highlighting the role of notch signaling in regulation of normal ventricular myocardial wall development. There were no deaths in patients with normal cardiac dimensions, function, and normal cardiac rhythm. Likewise, ventricular systolic function may initially deteriorate then improve, only to subsequently deteriorate later in life again (7). There may be variable degrees of ventricular dysfunction including well-preserved systolic function in antenatally diagnosed cases. There is some overlap with children who have more than three trabeculations but normal phenotype and normal left ventricular systolic and diastolic function. Echocardiographic assessment of ejection fraction using Simpson method in this population may be challenging given the extensive degree of trabeculations (137). Supraventricular and ventricular tachycardia are also reported findings on Holter or telemetry monitoring (152,153,154,155,156). Standard 2-D imaging demonstrates trabeculations and deep intertrabecular recesses or “valleys” in the left ventricle (Fig. The compacted layer should be clearly defined to allow accurate measurement of its dimensions. Axel reminds us that the papillary muscles join the network of trabeculae carneae lining the ventricular cavity, which is similar in appearance to noncompacted areas and could lead to a misdiagnosis (Fig. Moreover, false tendons and bands in the apical portion of the left ventricle are normal findings that could result in overdiagnosis (Fig. Although there remains some contention as to the specific criteria to fulfil the diagnosis, Jenni et al. Moreover, variability in the measurements is part of the accepted confusion and frustration pushing us to accept what we have today. Cardiac segmental analysis in left ventricular noncompaction: experience in a pediatric population. Solid arrows represent noncompact: compact ratio and broken arrows represent trabeculations. Our conclusion is that Jenni criteria endure the most appropriate standard if it is followed appropriately (10). Inclusion or exclusion of the trabeculations in the measurement remains contentious as discussed previously (Fig. The transmitral inflow pattern typically demonstrates a restrictive filling pattern with an elevated P. Tissue Doppler velocities typically show a reduction in Ea, Aa, and Sa velocities (137). Left ventricular noncompaction: a genetic cardiomyopathy looking for diagnostic criteria. Some of the cardiac segments with noncompacted areas could be evaluated using speckle tracking imaging for longitudinal strain. Although the majority of patients have noncompaction isolated to the left ventricle, biventricular involvement has been well documented (Video 54. Finally to avoid the overdiagnosis of this entity, the use of contrast echocardiography may prove very helpful (173,174). This may be particularly true in older adolescent patients, obese patients, or patients supported on mechanical ventilation (Figs. Contrast echocardiography may also define prominent false tendineae or apical bands (see Fig. Better border definition and improved visualization of the apex may improve measurement accuracy in these regions ( Videos 54. Delayed contrast hyperenhancement can also be utilized to assess perfusion defects and the presence of myocardial fibrosis (187,188,189,190,191,192). Patients with normal ejection fraction may require no medical treatment or just aspirin therapy.
The tail of the caudate nucleus continues where voluntary intended movements can occur from the body and arches downward and for- coincidently with involuntary unintended move- ward into the temporal lobe generic cyclophosphamide 50mg line medications ending in pril, where it eventu- ments cyclophosphamide 50 mg cheap medications you cant drink alcohol. The basal ganglia are the corpus striatum ally becomes continuous with the amygdaloid (in the cerebral hemisphere) cheap cyclophosphamide 50mg with visa treatment ringworm, the subthalamic nucleus (Fig generic cyclophosphamide 50 mg free shipping medicine used to stop contractions. The globus pallidus is located between The corpus striatum is subdivided anatomically the putamen and the internal capsule and is into the caudate and lentiform nuclei. These divided into lateral (outer) and medial (inner) two large nuclear masses are deep within the segments. Inferiorly, the putamen fuses with the the thalamus and lateral to the hypothalamus. In brain slices, the alter- dorsomedially, and (3) the subthalamic nucleus nate strands of gray and white matter provide ventrally (Fig. The subthalamic nucleus the striated appearance for which the corpus appears as a prominent biconvex structure nes- striatum was named. As a result, the corpus striatum consists a more dorsal compact part and a more ventral of the caudate nucleus, the putamen, and the reticular part. The compact part contains neu- globus pallidus structurally, but the striatum and rons flled with melanin, which accounts for the pallidum functionally (Fig. Reticular nigra neurons scattered through the most rostral part neurons are morphologically, physiologically, and of the cerebral crus and its continuation with the functionally identical to medial pallidal neurons. A Internal capsule Body of caudate nucleus Lateral view B B Dorsal section 8-2B C C Ventral section 8-2B Head of caudate nucleus Tail of caudate nucleus Putamen Amygdaloid nucleus Body of caudate nucleus B B Dorsal section 8-2B C C Ventral section 8-2B Head of caudate Medial view nucleus Accumbens Tail of caudate nucleus nucleus Putamen Amygdaloid nucleus Lat. Left lateral and right medial views of the corpus striatum and amygdaloid nucleus. Horizontal section through ventral level of corpus striatum (ant, anterior; cap, capsule; inf, inferior; int, internal; lat, lateral; med, medial; nucl, nucleus; post, posterior; vent, ventricle). Virtually all areas of Overview the cerebral cortex project in an orderly manner The basal ganglia link with the thalamus and to the striatum. These corticostriate projections cerebral cortex through a number of segregated reach the caudate nucleus and putamen directly topographically organized parallel circuits that from the adjacent white matter, most via the ante- subserve different functions. Corticostriatal circuit emphasized in this chapter focuses on projections from motor, premotor, and somatosen- pathways through the basal ganglia that regu- sory areas of the cerebral cortex project somato- late voluntary movements through thalamo- topically to the putamen. A thalamic input to the cortical projections to premotor, supplementary striatum arises in the intralaminar nuclei. The most important connections between indi- The connections of the basal ganglia (Fig. From the The pallidum and subthalamic nucleus are compact nigra arises the nigrostriatal projection, interconnected by the subthalamic fasciculus, which terminates in the caudate nucleus and a small bundle that intersects with the internal putamen in a manner reciprocal to the striatoni- capsule, where it separates these two nuclei. Pallidothalamic Limb projections Thalamic fasciculus Striatopallidal projection Subthalamic fasc. Subthalamic nucleus Inhibitory synapse Substantia nigra A Excitatory synapse Figure 8-8 A. Thalamic fasciculus Ansa lenticularis Subthalamic nucleus Compact Substantia Reticular nigra B Figure 8-8 (Continued) B. Position of pallidothalamic projections (ant, anterior; caps, capsule; fasc, fasciculus; int, internal; lat, lateral; med, medial; nucl, nucleus; post, posterior; vent, ventricle). The lenticular Extending from all parts of the striatum to all fasciculus arises from the dorsal surface of the parts of the pallidum are abundant striatopallidal medial pallidum (Fig. Striatopallidal projections can be either tially through the posterior limb of the internal direct or indirect. Medium spiny neurons with D1 capsule, and then passes through the subthala- receptors project to the medial pallidum, whereas mus where it is located between the subthalamic striatal neurons with D2 receptors project to the nucleus and zona incerta (Fig. The corticostriate and lenticularis arises from the ventral surface of the striatopallidal projections are topographically org- medial pallidum (Fig. Thus, ultimately, the is the medial pallidum, which exerts a strong basal ganglia infuence movements through the infuence on the thalamus. The pallidum and the reticu- in the ventral anterior nucleus and appear to be lar nigra inhibit the ventral anterior thalamic mainly concerned with head and eye movements. The ventral anterior nucleus activates the premo- tor cortex with glutamate as the neurotransmitter. This inhibition appears to have facilitatory effects on striatal neu- is differentially modulated by parallel activity in rons with D1 receptors and depressant effects on the direct and indirect pathways from the striatum others with predominately D2 receptors. Conversely, cortical rons and the suppression of undesired movements activation of other striatal neurons in the indirect by selective inhibition of other thalamocortical pathway results in striatal inhibition of lateral palli- projection neurons. Striatal neurons in the direct of the basal ganglia are the result of an imbalance pathway have D1 receptors that facilitate activity in activity in the direct and indirect pathways as in this circuit, whereas striatal neurons in the indi- a result of the loss of control normally exerted on rect pathway have D2 receptors that decrease activ- the striatum by the substantia nigra or on the pal- ity in the circuit. Cortical activation of the direct the cerebral cortex receives the sensory input, and pathway in due course disinhibits thalamic neurons its association areas generate the will to move. Concurrent a desired action and the concomitant suppression activation of the indirect pathway will lead to of conficting movements. The striatum permits inhibition of different thalamic neurons that may and controls movement through the chief efferent be involved in competing movement programs. Both are manifestations of the The premotor cortex programs complex voluntary “release” phenomena, the loss of pallidal inhibi- movements through connections with the motor tion of thalamic neurons. Honing of tone in basal ganglia disorders usually take the striatal and pallidal output occurs through recip- form of hypertonicity. In severe cases, there is rocal connections with the substantia nigra and rigidity in which the tone in all of the muscles the subthalamic nucleus, respectively. In such cases, the Abnormalities of the basal ganglia result in increased resistance to passive stretch is bidirec- negative and positive signs. The negative signs tional and occurs throughout the range of the are actions the patient wants to perform but can- movement. The frequency of the abnormal neurons can no longer elicit an activ- jerks corresponds to the frequency of the tremors. The positive signs occur because of the loss of The hypertonicity in this case is termed cogwheel control or the release of other parts of the motor rigidity. Dyskinesias Dyskinesias take the form of tremors, chorea, ath- Negative Signs etosis, ballismus, and tics. Tremors are rhythmic Negative signs of basal ganglia disease include or oscillatory movements in the distal parts of the akinesia, bradykinesia, and abnormal postural limbs, such as the hands. Akinesia refers to the hesitancy movements in the more distal parts of the limbs and in starting a movement and bradykinesia to the in the face. Athetosis is slow, writhing, or snake- slowness with which the movement is executed. Ballismus is violent Neither occurs because of paresis or paralysis; finging movements of the entire limb as a result these signs do not exist in basal ganglia disorders. Abnormal postural adjustments take the form Tics are stereotypical and repetitive movements of head and trunk fexion and the incapacity to involving several muscle groups simultaneously. A movements occur against the will of the patient form of abnormal postural adjustments is seen in and can neither be prevented from starting nor dystonia, in which unusual fxed postures occur interrupted once they do start. It is thought that altered occurs in Parkinson disease, also called paralysis impulse activity in the direct pathway results in agitans, the best-known basal ganglia disease and increased inhibition of thalamic neurons result- the disease described in the case at the beginning ing in decreased thalamocortical activity in of this chapter. The rigidity is more prominent in the Positive signs of basal ganglia disease include advanced stages of the disease.
In contrast cyclophosphamide 50mg lowest price medicine effexor, only 2% of atorvastatin is excreted through kidney cyclophosphamide 50 mg on line medications nurses; therefore safe cyclophosphamide 50 mg 4 medications list, it does not require any dose modification order cyclophosphamide 50 mg with amex treatment 8th march. Statins have been shown to reduce albuminuria, although studies using rosuvastatin have yielded conflicting results. Hypoglycemia in a patient with diabetes is defined as blood glucose <70 mg/dl, with or without adrenergic or neuroglycopenic symptoms. The blood glucose threshold to define hypoglycemia is higher in patients with diabetes as com- pared to nondiabetic individuals, where the cutoff is 55 mg/dl. This is because the threshold for activation of defense mechanisms against hypoglycemia is set at a higher level in diabetic individuals and higher threshold also provides time to the patient for taking action to prevent progression into neuroglycopenia. In addition, it provides a safety margin while using glucose monitoring devices, as these devices have limited accuracy at low plasma glucose levels. The initial adaptive response to hypoglycemia is cessation of insulin secretion at blood glucose of approximately 80–85 mg/dl. Symptoms of hypo- glycemia appear at blood glucose of 50–55 mg/dl, and cognitive dysfunction occurs at <50 mg/dl. These observations have been derived from hypoglycemic- hyperinsulinemic clamp studies in healthy individuals. This is because of severe endogenous insulin deficiency and impaired glucose–glucagon axis. The first line of defense against hypoglycemia is the decrease in insulin secretion with declining levels of glucose; however, this fails to occur in those with long- standing diabetes due to poor β-cell reserve. Further, in normal physiology, decrease in insulin secretion results in reduction of intra-islet insulin levels. This “∆ change” in intra-islet insulin is required for the stimulation of α-cells to secrete glucagon. Further, frequent episodes of hypoglycemia lead to sympathoadrenal failure (hypoglycemia-associated autonomic failure) result- ing in defective epinephrine secretion (third line of defense against hypoglyce- mia), thereby predisposing a patient to recurrent and severe hypoglycemia. Hypoglycemia is classified in patients with diabetes as severe (requiring assis- tance of another person), documented symptomatic (symptoms with spot glu- cose <70 mg/dl), asymptomatic (spot glucose <70 mg/dl without symptoms), probable symptomatic (symptoms without documentation of blood glucose), and relative hypoglycemia (symptoms with spot glucose >70 mg/dl). The importance of this classification is that it not only takes into account severe hypoglycemia, but also includes patients with a suspicion of hypoglycemia. In addition, it also helps to provide uniformity in defining hypoglycemia as an adverse event with antidiabetic drugs in scientific studies. Patients with hypoglycemia presenting only with adrenergic symptoms should be treated with oral glucose tablets or fruit juice or candy, irrespective of blood glucose levels. Blood glucose should be re-estimated after 15–20 min, and fail- ure of normalization of blood glucose requires further administration of oral glucose/carbohydrates. Patients receiving basal insulin or long-acting sulfonyl- ureas (glibenclamide or glimepiride) require close monitoring for at least 24–72 h. Patients with hypoglycemia along with cognitive dysfunction should be administrated 25 g of dextrose (25% dextrose, 100 ml) intravenously to rap- idly normalize blood glucose and may require continuous administration of 5% dextrose, depending upon improvement in sensorium and antidiabetic treat- ment received. Blood glucose should not be allowed to overshoot >200 mg/dl, as rapidly rising blood glucose may lead to cerebral dehydration and further worsening of sensorium. Intravenous dextrose should be discontinued only when patient starts taking orally, as hepatic glycogen stores are repleted only with oral intake. After recovery from the episode, an active search should be made to explore the cause of hypoglycemia 48. Infections are more severe and aggressive in patients with diabetes; however, it is still debatable whether diabetes per se increases the risk of infections. Cutaneous candidiasis is the most common infection, followed by urinary tract infection and pneumonia. Hyperglycemic milieu, altered leukocyte function, and increased oxidative stress contribute to more severe and aggressive infections in diabetes. Are microorganisms causing emphysematous pyelonephritis and emphy- sematous cholecystitis same? Emphysematous cholecystitis is caused by Clostridia, which is a commensal in the intestinal tract. Autonomic neuropathy is associated with impaired absorp- tion of micronutrients from the gastrointestinal tract. Metformin impairs calcium channel-mediated B12 absorption in distal small intestine and contribute to macrocytic anemia. Pioglitazone results in ane- mia due to hemodilution and preferential diversion of primitive mesenchymal stem cells to adipocytes rather than to erythropoietic stem cells. Occult gastrointestinal bleed is not uncommon in patients with diabetes as antiplatelet drugs are frequently used in these patients. Abdominal pain and vomiting can occur in a patient with diabetes due to diabetic ketoacidosis, acute pancreatitis, acute cholecystitis, acute papillary necrosis, gastroparesis, and diabetic kidney disease. Further, hyperglycemia due to pregnancy usu- ally manifests at 24–28 weeks of gestation, while preexisting diabetes may manifest even during first trimester. This differentiation is important as women with preexisting diabetes are more likely to have fetal malformations, need evaluation and monitoring for diabe- tes-specific complications. In addition, this definition does not entail absolute numerical values of plasma glucose to define hyperglycemia during pregnancy as opposed to the diagnosis of diabe- tes in nonpregnant population. Fuel-mediated teratogenesis refers to teratopathy occurring due to exposure of embryo or fetus to the unfavorable milieu of metabolic fuels such as high levels of glucose and ketones. The type and severity of defects depend on the time of gestation at which the embryo/fetus has been exposed. If the exposure to high levels of glucose occurs during embryogenesis (<8 weeks of gestation), it results in diabetic embryopathy, as seen in patients with uncontrolled preexisting diabe- tes. However, if fetus (after 8 weeks of gestation) is exposed to this abnormal metabolic milieu, then anthropometric and metabolic abnormalities predominate the clinical picture, rather than embryopathy. Diabetic embryopathy is a result of peri-conceptional uncontrolled hyperglyce- mia which influences organogenesis during embryonic period. The congenital anomalies associated with diabetic embry- opathy include neural tube defects, caudal regression syndrome, transposition of great vessels, ventricular septal defect, hypoplastic left heart syndrome, renal agenesis, duodenal atresia and hypoplastic femur. Out of these numerous anom- alies, neural tube defects are the most common, while the diabetes-specific defect is caudal regression syndrome (sacral agenesis). The prime pathogenetic mechanism implicated in congenital malformation is the exposure of embryo to hyperglycemia, hyperketonemia (3 β-hydroxybutyrate), and metabolites like inositol, sorbitol, and arachidonic acid. Every pregnant woman should be screened for hyperglycemia as early as pos- sible (first contact visit or preferably <12 weeks); if not, there is a probability of missing preexisting diabetes. If the screening test is negative at first trimester, retesting is recommended in all women between 24 and 28 weeks of gestation. The retesting at 24–28 weeks is recommended as insulin resistance peaks at this time due to rising concentration of progesterone, human placental lactogen, prolactin, cortisol, and growth hormone. The aim of screening at first trimester is to recognize those women with preex- isting diabetes. There are two approaches to screen for hyperglycemia at 24–28 weeks of gesta- tion: a one-step approach or two-step approach. The risk to mother and fetus starts even at a fasting plasma glucose >75 mg/dl, 1-h plasma glucose >106 mg/dl and 2-h plasma glucose of >91 mg/ dl after 75-g glucose load.
Syndromes
- Regional (spinal or epidural) anesthesia. Medicine is put into your back to make you numb below your waist. You will also get medicine to make you sleepy. And you may get medicine that will make you forget about the procedure, even though you are not fully asleep.
- Biopsy of affected tissue
- Gastrointestinal problems
- Family therapy
- Seizures
- What other symptoms do you have?
- Lead bullets, fishing sinkers, curtain weights.
- Androgens
Guidelines and standards for performance of a pediatric echocardiogram: a report from the Task Force of the Pediatric Council of the American Society of Echocardiography purchase cyclophosphamide 50mg without a prescription medicine abuse. Hemodynamic determinants of the peak systolic left ventricular-aortic pressure gradient in children with valvar aortic stenosis buy discount cyclophosphamide 50mg line 7 medications that can cause incontinence. Continuous-wave Doppler echocardiographic assessment of severity of calcific aortic stenosis: a simultaneous Doppler-catheter correlative study in 100 adult patients buy 50 mg cyclophosphamide symptoms 6 week pregnancy. Non-invasive estimation of the mean pressure difference in aortic stenosis by Doppler ultrasound generic cyclophosphamide 50 mg medicine just for cough. Usefulness of the Doppler mean gradient in evaluation of children with aortic valve stenosis and comparison to gradient at catheterization. Clinical utility of Doppler echocardiography in assessing aortic stenosis severity and predicting need for intervention in children. Value of three-dimensional speckle-tracking in detecting left ventricular dysfunction in patients with aortic valvular diseases. Strain analysis in patients with severe aortic stenosis and preserved left ventricular ejection fraction undergoing surgical valve replacement. Comparison between different speckle tracking and color tissue Doppler techniques to measure global and regional myocardial deformation in children. Left ventricular outflow tract obstruction: an indication for intraoperative transesophageal echocardiography. Midwall fibrosis is an independent predictor of mortality in patients with aortic stenosis. Hemodynamic responses to ergometer exercise in children and young adults with left ventricular pressure or volume overload. Exercise electrocardiogram, blood pressure, and working capacity in young patients with valvular or discrete subvalvular aortic stenosis. Indications for cardiac catheterization and intervention in pediatric cardiac disease: a scientific statement from the American Heart Association. Natural history of mild congenital aortic stenosis elucidated by serial hemodynamic studies. Natural history of unoperated aortic stenosis during a 50-year period of cardiac valve replacement. Rapid evolution from “normal” left ventricular outflow tract to fatal subaortic stenosis in infancy. Natural history and surgical outcomes for isolated discrete subaortic stenosis in children. Development and validation of an echocardiographic model for predicting progression of discrete subaortic stenosis in children. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Introduction: eligibility recommendations for competitive athletes with cardiovascular abnormalities-general considerations. Long-term outcome of patients with isolated thin discrete subaortic stenosis treated by balloon dilation: a 25-year study. Balloon dilation of the aortic valve: studies in normal lambs and in children with aortic stenosis. Balloon aortic valvuloplasty: results of the Valvuloplasty and Angioplasty of Congenital Anomalies Registry. Comparison of single and double balloon valvuloplasty in children with aortic stenosis. Balloon valvuloplasty for recurrent aortic stenosis after surgical valvotomy in childhood: immediate and follow-up studies. Balloon dilatation of congenital aortic valve stenosis in infants and children: short term and intermediate results. Independent predictors of immediate results of percutaneous balloon aortic valvotomy in children. Effectiveness of balloon valvuloplasty in the young adult with congenital aortic stenosis. Clinical and hemodynamic follow-up after percutaneous aortic valvuloplasty in the elderly. Early restenosis following successful percutaneous balloon valvuloplasty for calcific valvular aortic stenosis. Follow-up results of balloon aortic valvuloplasty in children with special reference to causes of late aortic insufficiency. Aortic valve reinterventions after balloon aortic valvuloplasty for congenital aortic stenosis intermediate and late follow-up. Twenty-five year experience with balloon aortic valvuloplasty for congenital aortic stenosis. Intermediate-term effectiveness of balloon valvuloplasty for congenital aortic stenosis. Surgical valvuloplasty versus balloon aortic dilation for congenital aortic stenosis: are evidence-based outcomes relevant? Surgical valvotomy and repair for neonatal and infant congenital aortic stenosis achieves better results than interventional catheterization. In a series of 123 consecutive neonates and infants with severe aortic stenosis, balloon valvuloplasty was associated with decreased freedom from reintervention compared to surgical valvuloplasty, though mortality and longterm freedom from valve replacement were similar between groups. Repeat balloon aortic valvuloplasty effectively delays surgical intervention in children with recurrent aortic stenosis. Aortic valve morphology is associated with outcomes following balloon valvuloplasty for congenital aortic stenosis. Balloon dilation of severe aortic stenosis in the fetus: potential for prevention of hypoplastic left heart syndrome: candidate selection, technique, and results of successful intervention. Aortic valvuloplasty in the fetus: technical characteristics of successful balloon dilation. Fetal aortic valve stenosis and the evolution of hypoplastic left heart syndrome: patient selection for fetal intervention. Predictors of technical success and postnatal biventricular outcome after in utero aortic valvuloplasty for aortic stenosis with evolving hypoplastic left heart syndrome. Fetal intervention for critical aortic stenosis: advances, research and postnatal follow-up. Fetal aortic valvuloplasty for evolving hypoplastic left heart syndrome: postnatal outcomes of the first 100 patients. Of 100 patients who underwent fetal aortic valvuloplasty, there were 88 live births, 38 of whom eventually received a biventricular repair. Fetal mortality was 11%, while valvuloplasty was technically successful in 77% of cases. Estimated survival of the entire fetal cohort was 75±5% at 5 years, with improved survival in patients with a technically successful valvuloplasty. Current perspective on aortic valve repair and valve-sparing aortic root replacement. Is there still a place for open surgical valvotomy in the management of aortic stenosis in children?
Cyclophosphamide 50 mg generic. PMX - Dark Days (full album listen).