
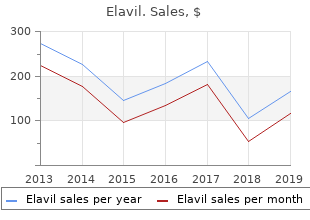
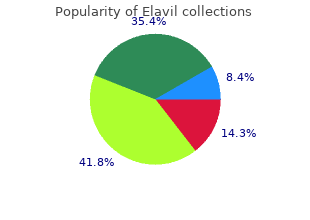
Oberlin College. V. Joey, MD: "Purchase online Elavil - Safe Elavil online OTC".
Sub- to-rostral trend during early brain sequently cheap 25 mg elavil free shipping foot pain tendonitis treatment, the three eigenvalues/eigenvectors development cheap 50mg elavil fast delivery cape fear pain treatment center dr gootman. After the the fiber bundles associated with language and completion of neuronal migration during the last sensorimotor functions buy generic elavil 75 mg brunswick pain treatment center brunswick ga, whereas gender trimester of gestation 75mg elavil with mastercard pain medication for small dogs, interneuron connections effects are subtle during infancy. Indeed, regardless of different diffusion parame- of Major White Matter Tracts ters, results reported in the literature have gener- Measurements of intracranial gray matter, and ally converged on a nonlinear developmental trend. With these microstructural developments, it tropy of the underlying water diffusion within a is highly plausible that water diffusion will be given voxel, it does not separately evaluate water modified owing to the alteration of the biological diffusion parallel or perpendicular to the long axis microenvironment (barriers) such that a similar of axonal bundles. Red/yellow/green regions of interest are shown for illustration of the relative significance in age-dependent development (red: p<0. The experimentally measured Life values of the 1- and 2-year-old groups are normalized to those of the neonates. Subse- water diffusivity parallel and perpendicular to the quently, a slower, adult-like level of axonal devel- main axis of water diffusion, respectively, poten- opment was observed beyond 17 postnatal tially offering additional insights into the micro- months (1. The linear ani- fusivity measures for a better depiction of the sotropy is defined as the trace normalized complex underlying microstructural changes dur- difference between the primary and second eigen- ing the first 2 years of life. Similar findings were observed bilateral uncinate fasciculus tracts, inferior longi- using tract-based analysis19; callosal bundles show tudinal fasciculus, and arcuate fasciculus tracts. Horizontal lines repre- sent the overall mean of the average values in one age group. Geng et sory functions requires either rapid up-down in- al29 studied the genetic and environmental effects formation relaying through center projection on the spatiotemporal growth of different major fibers (e. This conclusion is with the anterior–posterior limb of the internal also consistent with the lower heritability esti- capsule, the external capsule may have started mates reported in adults than in pediatric subjects. In general, the authors observed sub- (genu, anterior and superior thalamic radiations, stantial heritability of diffusion properties during anterior cingulum, arcuate fasciculus, temporal– infancy, which is higher than that reported in parietal segment) (▶ Fig. The sig- understanding cognitive development in early nificant positive correlation between heritability infancy. In the adult brain, language and handedness are among the most well recognized brain functional lateralization. Aiming ing early brain development, likely due to the lack to address this question, Dubios et al37 examined of robust cognitive assessment strategies for such the whole brain diffusion properties in infants young ages. Mean convincing evidence on the lateralization of diffu- apparent diffusion coefficient values at the level of sion property early in life that might be critical to the centrum semiovale were determined at term- the later lateralization of corresponding functions. Scatter plots highlight examples of significant associations between infants’ working memory and key white matter tracts: genu, arcuate, and anterior cingulum. Only the left (L) arcuate and left cingulum are shown above; however, scatter plots for these tracts in the right hemisphere are very similar. Therefore, more studies are needed to devastating genetic disease, Krabbe disease, unre- delineate the potential mechanisms of the lated umbilical cord transplantation, the only observed sex differences in diffusion in adults. The red triangles represent the six patients with Krabbe disease, whereas the blue diamonds show the typical controls. The red and blue lines represent the linear trend related to the corrected age at the time of the magnetic resonance imaging. Temporally, dif- showed significant differences in the corticospinal ferent diffusion properties follow nonlinear tracts of asymptomatic neonates who had the growth featuring the most significant changes dur- early-onset form of Krabbe disease. During this time period, Krabbe through statewide neonate screening pro- significant genetic effects on the development of grams. Quantitative tract-based References white matter development from birth to age 2years. Mapping infant brain 2011; 198(3): 173–175 myelination with magnetic resonance imaging. White and gray matter 83–84 development in human fetal, newborn and pediatric brains. Distinct ment in the cerebral white matter of the human fetus and genetic influences on cortical surface area and cortical infant. Genetic control netic resonance imaging of brain development in prema- over the resting brain. White matter her- 2002; 23(9): 1445–1456 itability using diffusion tensor imaging in neonatal brains. Spinogenesis and pruning scales Twin Res Hum Genet 2012; 15(3): 336–350 across functional hierarchies. Concurrent overproduction of synapses in diverse Exp Neurol 1988; 47(3): 217–234 regions of the primate cerebral cortex. Biochim Biophys Acta 2012; tions of basal dendritic trees of pyramidal neurons in the 1822(3): 386–400 human prefrontal cortex: a layer-specific pattern. White matter Cortex 2008; 18(4): 915–929 damage on diffusion tensor imaging correlates with age- [14] Flechsig P. Associations between related cellular compartments in the human cerebral wall as white matter microstructure and infants’ working memory. Structural asymmetries in the infant Radiology 2003; 229(3): 673–681 language and sensori-motor networks. Changes in white detects abnormalities in the corticospinal tracts of neonates matter microstructure during adolescence. If water molecules migrate during the more subtle age-related changes in white mat- interval between these gradients, then signal loss ter integrity, and these methods may enable the will occur. Such signal loss represents uninhibited differentiation of normal adult aging from mild random diffusion of water molecules representing cognitive impairment and Alzheimer dementia. Diffusion restriction represents ● White matter indices are more sensitive to subtle constriction of water molecules preventing ran- changes than anatomical volumetric analyses dom motion between gradient pulses and present- examining atrophy in a variety of dementias. The extent to which white matter premise of water diffusion changes as an indirect tracts are maintained indirectly influences water indicator of underlying brain parenchyma. Multiple methods are available for examining the multidirectional data acquired by diffusion tensor imaging. These and other newer analytic techni- standard deviation of the three diffusivities) ques are being applied to the study of the aging where the value ranges from isotropic (0), a brain. Determining whether worsening reac- vide insight into the mechanisms by which cogni- tion time or memory is related to mild cognitive tive functions are disrupted. Elucidating the basis impairment or “old age” versus a more debilitating of cognitive decline is an important problem in the dementia, such as Alzheimer disease, provides clinical assessment of elderly individuals, which is important information for patients and their fami- becoming of pressing concern in most developed lies and can guide appropriate treatment strat- countries where aging demographics are egies. More recent vulnerable to healthy myelin formed by oligoden- studies offer evidence to support the use of single- drocytes earlier in life. Both abnormal and normal adult aging may varying stages on the aging–cognitive decline– lead to significant decline in white matter organi- dementia spectrum (the definitions of which differ zation. Other variables, including white matter volume or hyperintense lesions, did not explain Association between Specific this relationship. In callosum, superior longitudinal fasciculus, and addition, these findings are robust for the specific inferior fronto-occipital fasciculus). Normal axon integrity exhibits a dense, rich microstructure with normal myelination and little extracellular space. In comparison, the aging brain demonstrates axonal loss and dysmyelination that results in thinning of the myelin sheath and increased extracellular space.
Diseases
- Heterotaxy, visceral, X-linked
- Scoliosis
- Phocomelia ectrodactyly deafness sinus arrhythmia
- Ambral syndrome
- Blue diaper syndrome
- Short bowel syndrome
- Crome syndrome
- Uniparental disomy of 14
Early elective tracheal intubation is advis- 11 200–300 times the afnity of oxygen for hemoglo- able when there are obvious signs of heat bin buy 75mg elavil amex pain treatment germany. Patients with hoarseness and globin to form carboxyhemoglobin purchase elavil 50mg free shipping pain treatment for carpal tunnel syndrome, it decreases the stridor require immediate intubation; emergency afnity of the other binding sites for oxygen elavil 10mg free shipping pain treatment satisfaction scale, shif- cricothyrotomy or tracheostomy is necessary if oral ing the hemoglobin dissociation curve to the right purchase elavil 75 mg on line pain medication for dying dogs. The net result is a marked reduction in the oxygen- The presence of clinically important carbon carrying capacity of blood. The diag- Clinical manifestations result from tissue hypoxia nosis of carbon monoxide poisoning requires coox- from impaired oxygen delivery. Levels greater than imetry: pulse oximeters cannot reliably diferentiate 20–40% carboxyhemoglobin are associated with between carboxyhemoglobin and oxyhemoglobin. Lower levels may also produce with 100% oxygen; some clinicians advocate hyper- symptoms because carbon monoxide also binds baric oxygen therapy if the patient does not respond cytochrome c and myoglobin. The diagnosis of cyanide poison- anisms include increased cardiac output and periph- ing is difcult because reliable measurements of eral vasodilation. The enzyme rhodanase normally con- to fumes from fres that contain synthetic materi- verts cyanide to thiocyanate, which is subsequently als, particularly those containing polyurethane. Treatment for severe cyanide, which may be inhaled or absorbed through cyanide toxicity consists of administering sodium mucosal surfaces and skin, binds the cytochrome nitrite, 300 mg intravenously as a 3% solution over system of enzymes and inhibits cellular production 3–5 min, followed by sodium thiosulfate, 12. Patients present intravenously in the form of a 25% solution over with neurological impairment and lactic acidosis; 1–2 min. Sodium nitrite converts hemoglobin to they typically have arrhythmias, increased cardiac methemoglobin, which has a higher afnity for cya- output, and marked vasodilation. Infammation of the airways results shunting should be managed with tracheal intuba- in bronchorrhea and wheezing. Relief of the ischemia with other forms of acute lung injury, nosocomial in these areas can restore contractile function, albeit infectious pneumonias are common. Stunning may be observed follow- ing aortic cross-clamping during cardiopulmonary bypass and present as a reduced cardiac output upon attempted separation from bypass (see Chapter 22). With positron emission tomography, or by showing that recent advances in interventional cardiology, the in- the hypocontractile myocardium responds to dobu- hospital mortality rate has been reduced to less than tamine during stress echocardiography. Coronary inversely proportionate to the extent of necrosis, emboli or severe spasm is less commonly the cause. Based on distribution of the obstructed vessel and whether local resources, timing, and anatomic fndings dur- collateral vessels have formed. Anterior, apical, and ing angiography, angioplasty, stenting, or coronary septal infarcts of the lef ventricle are usually due to artery bypass surgery may be preferred. All patients rhage, and less commonly follows coronary plaque without contraindications (such as acute heart fail- rupture and thrombosis. If angina persists or if there is a thought to occur in areas adjacent to infarcted contraindication to β blockers, calcium chan- myocardium and can contribute to ventricular nel blockers should be administered. Renal lar tachycardia, if treated medically is best managed hypoperfusion typically the result of decreased arte- with amiodarone (150 mg intravenous bolus over rial perfusion pressure, markedly increased venous 10 min). Synchronized cardioversion may be used pressure, or renal vasoconstriction (Table 57–7 ). Patients with paroxysmal supraventricular Tese hormones constrict cutaneous muscle and tachycardia, whose ejection fraction is preserved, splanchnic vasculature and promote salt and water should be treated with a calcium channel blocker, a retention. Moreover, the diagnosis of renal Postrenal azotemia is one of exclusion; thus, prerenal and Urethral obstruction postrenal causes must always be excluded. How- Bladder outlet obstruction Neurogenic bladder ever, not all patients with acute azotemia have kid- Bilateral ureteral obstruction ney failure. Likewise, urine output of more than Intrinsic 500 mL/d does not imply that renal function is nor- Calculi mal. Exclusion of postre- Fractional excretion <1 >3 Variable nal azotemia requires physical diagnosis and imag- of sodium (%) ing, whereas exclusion of prerenal azotemia depends Renal failure index <1 >1 Variable on the response to treatments aimed at improving renal perfusion. Diagnosis and treatment may be facilitated by analysis of urine (see Table 57–8); uri- help maintain glomerular fltration. The ability is preserved and refected by a low urinary diagnosis of prerenal azotemia is usually suspected sodium concentration and high urine/serum creati- from the clinical setting and confrmed by urinary nine ratio. The hepatorenal syn- Urine creatinine/serum creattinine drome is discussed in Chapter 33. Obstruction of urinary fow failure index, which is the urinary sodium concen- from both kidneys is usually necessary for azotemia tration divided by the urine/plasma creatinine ratio, and oliguria/anuria in these conditions. Rapid diagnosis sodium concentration as a measure of tubular func- and relief of acute obstruction usually restore nor- tion. Moreover, intrinsic kidney diseases that pri- mal renal function, ofen accompanied by a diure- marily afect renal vasculature or glomeruli may not sis. Obstruction may be diagnosed by a physical afect tubular function and therefore are associated examination (the upper margin of the bladder can with indices that are similar to prerenal azotemia. Inadequate oxygen deliver to trast dyes, and cyclosporine also appear to produce the kidney is the likely triggering event, leading direct intrarenal vasoconstriction. Hemoglobin to aferent arteriolar constriction, decreased glo- and myoglobin are potent nephrotoxins when merular permeability, increased vascular perme- they are released during intravascular hemolysis ability, altered coagulation, infammation, leukocyte and rhabdomyolysis, respectively. Cyclooxygenase activation, direct epithelial cell injury, and tubular inhibitors, particularly nonsteroidal antiinfam- obstruction from intraluminal debris or edema. All matory drugs, may play an important role in at can decrease glomerular fltration. Inhibition of prostaglandin fltered solutes through damaged portions of renal tubules may allow reabsorption of creatinine, urea, and other nitrogenous wastes. In some studies, nonoliguric patients also and burns) appear to have a lower complication rate and to Radiographic contrast agents require shorter hospitalizations. Teoretically, Organic solvents the resulting increase in urinary output might be Myeloma protein therapeutic by preventing tubular obstruction. Diuret- to metabolic acidosis, fuid overload, and hyperkale- ics continue to be useful for conventional medical mia. Nevertheless, recent clinical trials have failed to indications (eg, pulmonary edema or rhabdomy- show beneft of continuous technique over intermit- olysis). Daily weight measurements help guide fuid that nutrition should be provided, and 1. Sodium and potassium intake is limited of protein can be given, particularly for patients on to 1 mEq/kg/d. Hyperkalemia may require admin- istration of an ion-exchange resin (sodium polysty- rene), glucose and insulin, calcium gluconate, or Infections & Sepsis sodium bicarbonate. Sodium bicarbonate therapy may also be necessary for metabolic acidosis when The systemic infammatory response to infec- the serum bicarbonate level decreases to less than tion, termed sepsis syndrome ( Figure 57–8 ), does 15 mEq/L. Hyperphosphatemia requires dietary not necessarily indicate the presence of bactere- phosphate restriction and phosphate binders such mia. Moreover, the infammatory response is not as sevelamer, aluminum hydroxide, calcium carbon- unique to severe infections: similar manifestations ate, calcium acetate. Renal replacement therapy may be employed to treat or prevent uremic complications (see Bacteremia Table 30–6). Dialysis does not appear to hasten recovery but Burns may in fact aggravate kidney injury if hypotension Fungemia occurs or too much fuid is removed. Severe Altered mental status sepsis exists when these features are associated Significant edema or positive fluid balance (>20 mL/kg over 24 h) with organ dysfunction.
Syndromes
- Sinus infection
- High blood pressure (hypertension)
- The baby begins to store fat.
- Breast MRI scan
- Diarrhea
- HCG urine test
Techniques & Complications Respiratory Gas A precordial stethoscope (Wenger chestpiece) is a Exchange Monitors heavy discount elavil 50mg ayurvedic back pain treatment kerala, bell-shaped piece of metal placed over the chest or suprasternal notch buy elavil 75 mg cheap advanced pain treatment center jackson tn. Various chestpieces are available buy elavil 75 mg low cost chronic pain treatment vancouver, but the child Indications size works well for most patients order 75 mg elavil amex pain medication for little dogs. The bell is con- Prior to the routine availability of gas exchange nected to the anesthesiologist by extension tubing. Likewise, the heart tones could be heart sounds is much better than with a precordial auscultated to confrm a beating heart. Specifcally, oxyhemoglobin (HbO2 ) absorbs more infrared light (940 nm), whereas deoxyhemo- Thermocouple Connection to globin absorbs more red light (660 nm) and thus temperature appears blue, or cyanotic, to the naked eye. The ratio of the absorptions at the red and infrared wavelengths is analyzed by a microprocessor to pro- instead of the esophagus, resulting in a gas leak vide the oxygen saturation (Spo2) of arterial blood around the tracheal tube cuf. The greater the ratio of red/ infrared absorption, the lower the arterial satu- Clinical Considerations ration. Arterial pulsations are identifed by plethys- mography, allowing corrections for light absorption The information provided by a precordial or esoph- by nonpulsating venous blood and tissue. Heat from ageal stethoscope includes confrmation of ventila- the light source or sensor pressure may, rarely, result tion, quality of breath sounds (eg, stridor, wheezing), in tissue damage if the monitor is not periodically regularity of heart rate, and quality of heart tones moved. The confrmation of bilateral breath sounds afer tracheal intubation, however, is made with a binaural stethoscope. Techniques & Complications 100 Pulse oximeters combine the principles of oximetry 50 and plethysmography to noninvasively measure oxygen saturation in arterial blood. A sensor con- taining light sources (two or three light-emitting 10 diodes) and a light detector (a photodiode) is placed across a fnger, toe, earlobe, or any other perfused 550 650 750 850 950 tissue that can be transilluminated. When the light (Red) (Infrared) source and detector are opposite one another across the perfused tissue, transmittance oximetry is used. The for- mer requires the placement of a pulmonary artery In addition to Spo2, pulse oximeters provide an catheter containing fberoptic sensors that continu- indication of tissue perfusion (pulse amplitude) and ously determine Svo2 in a manner analogous to measure heart rate. Because Svo2 varies with changes in to 100%, only gross abnormalities are detectable in hemoglobin concentration, cardiac output, arterial most anesthetized patients. Depending on a particu- oxygen saturation, and whole-body oxygen con- lar patient’s oxygen–hemoglobin dissociation curve, sumption, its interpretation is somewhat complex. Tis compares with clinically detect- fberoptic sensor in the internal jugular vein, which able cyanosis, which requires 5 g of desaturated provides measurements of jugular bulb oxygen satu- hemoglobin and usually corresponds to an Spo2 of ration in an attempt to assess the adequacy of cere- less than 80%. Unlike pulse oximetry, brain oximetry mea- register a falsely high reading in patients with car- sures venous and capillary blood oxygen saturation bon monoxide poisoning. Tus, its same absorption coefcienThat both red and infra- oxygen saturation readings represent the average red wavelengths. The resulting 1:1 absorption ratio oxygen saturation of all regional microvascular corresponds to a saturation reading of 85%. Cardiac arrest, methemoglobinemia causes a falsely low satura- cerebral embolization, deep hypothermia, or severe tion reading when Sao2 is actually greater than hypoxia cause a dramatic decrease in rSo2. Most pulse oximeters are inaccurate at low Spo2, and all demonstrate a delay between changes in Sao2 and Sp o2. A rapid fall of Etco2 is a leakage of light from the light-emitting diode to sensitive indicator of air embolism, a major com- the photodiode, bypassing the arterial bed (opti- plication of sitting craniotomies. In the recovery room, pulse Capnography is a valuable monitor of the pul- oximetry helps identify postoperative pulmonary monary, cardiovascular, and anesthetic breathing problems, such as severe hypoventilation, broncho- systems. Tus, they were incapable Diverting (sidestream) capnographs continuously suctions gas from the breathing circuit into a sample cell within the monitor. High aspiration rates (up to transducer 250 mL/min) and low-dead-space sampling tubing usually increase sensitivity and decrease lag time. If tidal volumes (Vt) are small (eg, pediatric patients), however, a high rate of aspiration may entrain fresh gas from the circuit and dilute Etco2 measure- ment. Low aspiration rates (less than 50 mL/min) can retard Etco2 measurement and underestimate it during rapid ventilation. To gas) is proportional to the amount of the unknown minimize the error introduced by nitrous oxide, gas. Oxygen and nitrogen do not absorb infrared various modifcations and flters have been incorpo- light. Capnographs rap- devices that use a single- or dual-beam infrared light 1 source and positive or negative fltering. Because idly and reliably indicate esophageal intubation—a common cause of anesthetic catastro- oxygen molecules do not absorb infrared light, their phe—but do not reliably detect bronchial intuba- concentration cannot be measured with monitors tion. Piezoelectric Analysis caused by malignant hyperthermia causes a marked The piezoelectric method uses oscillating quartz rise in Etco2. Volatile The gradient between Paco2 and E tco 2 (nor- anesthetics dissolve in the lipid layer and change the mally 2–5 mm Hg) refects alveolar dead space frequency of oscillation, which, when compared with (alveoli that are ventilated but not perfused). Any the frequency of oscillation of an uncovered crystal, signifcant reduction in lung perfusion (eg, air allows the concentration of the volatile anesthetic embolism, decreased cardiac output, or decreased to be calculated. Tere are Galvanic cell (fuel cell) contains a lead anode and no contraindications to analyzing these gases. No plateau gas during part of the inspiratory cycle signals the is reached before the next inspiration. Because the lead electrode is con- resulting change in volume (or pressure or fow) to sumed, monitor life can be prolonged by exposing it a known standard, the amount of oxygen can be to room air when not in use. Paramagnetic Analysis cathode and a silver anode, both bathed in an elec- Oxygen is a nonpolar gas, but it is paramagnetic, trolyte, separated from the gas to be measured by and when placed in a magnetic feld, the gas will a semipermeable membrane. The amount of cur- A End rent that fows between the anode and the cathode is inspiration Expiration proportional to the amount of oxygen present. Spirometry Newer anesthesia machines can measure (and Inspiration therefore manage) airway pressures, volume, and fow to calculate resistance and compliance and to display the relationship of these variables as fow (ie, volume or pressure–volume loops). Measurements Pressure of fow and volume are made by mechanical devices B that are usually fairly lightweight and are ofen Exhalation placed in the inspiratory limb of the anesthesia circuit. The most fundamental measurements include low peak inspiratory pressure and high peak inspi- ratory pressure, which indicate either a ventilator or circuit disconnect, or an airway obstruction, respec- tively. If a normal loop is observed shortly afer induction of anesthesia and a subsequent loop is dif- ferent, the observant anesthesiologist is alerted to the fact that pulmonary and/or airway compliance Techniques & Complications may have changed. Electrode position (montage) is governed by the international 10–20 system (Figure 6–7 ). Tere are no centrating individuals, and at times, in individuals contraindications. Some studies have demonstrated a reduced in sleeping individuals and during anesthesia. Moreover, many monitors have a delay, ischemia, such as during carotid endarterectomy as which might only indicate a risk for the patient being well as during epilepsy surgery. The readings shown waves in decreasing frequencies (γ, more than 30 hertz represent examples of possible readings that may be seen [Hz]; β ,12–30 Hz; α , 8–12 Hz; θ , 4–8 Hz; δ, 0–4 Hz); K, K in conjunction with each frontal electroencephalography complexes; Lat, latency between an auditory stimulus trace. Bispectral analysis may reduce thousand dollars and the electrodes are approxi- patient awareness during anesthesia, an issue that is mately $10 to $15 per anesthetic and cannot be important to the public. More recently the monitor converts the Narcotrend stages into a dimensionless number from 0 (asleep) to 100 (awake) by nonlinear regression.