
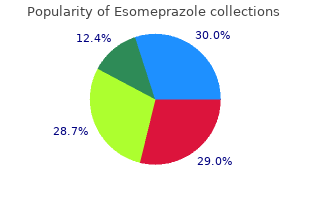
Bellarmine University. D. Xardas, MD: "Purchase online Esomeprazole cheap - Cheap Esomeprazole online".
Salmonella ser Typhi is classifed occur cheap esomeprazole 40 mg visa gastritis diet 4 you, and focal infections are recognized in in O serogroup D quality esomeprazole 20 mg gastritis symptoms lower abdominal pain, along with many other as many as 10% of patients with nontyphoidal common serovars 20mg esomeprazole fast delivery gastritis snacks, including Enteritidis and Salmonella bacteremia cheap esomeprazole 40mg line gastritis or pancreatic cancer. In 2011, the most commonly reported In the United States, the incidence of invasive human isolates in the United States were Salmonella infection is highest among infants. Salmonella serovars Enteritidis, Typhimurium, Certain Salmonella serovars (eg, Dublin, Newport, Javiana, and Heidelberg; these 5 Typhi, Choleraesuis), although rare, are serovars generally account for nearly half of more likely to result in invasive infection than all Salmonella infections in the United States. However, in recent years in The relative prevalence of other serovars varies sub-Saharan Africa, certain serovars of non- by country. Approximately 75% to 95% of the typhoidal Salmonella have been reported to be serovars associated with invasive pediatric dis- common. Notably, these highly lethal African ease in sub-Saharan Africa are S Typhimurium nontyphoidal Salmonella organisms are geneti- (Table 120. The major food a protracted bacteremic illness referred to, vehicles of transmission to humans in industri- respectively, as typhoid and paratyphoid fever alized countries include food of animal origin, and, collectively, as enteric fevers. In the current taxonomy, only 2 species are recognized, Salmonella entericaand Salmonella bongori. S entericahas 6 subspecies, of which subspecies I (enterica) contains the overwhelming majority of all Salmonellapathogens that affect humans, other mammals, and birds. Serotypes are now written nonitalicized with a capital frst letter (eg, Typhi, Typhimurium, Enteritidis). The serotype of Salmonellais determined by its O (somatic) and H (fagellar) antigens and whether Vi is expressed. Reptiles rates of invasive infections and mortality are and amphibians that live in tanks or aquari- higher in infants, elderly people, and people ums can contaminate the water. Small turtles with hemoglobinopathies (including sickle with a shell length of less than 4 inches are a cell disease) and immunocompromising well-known source of human Salmonella infec- conditions (eg, malignant neoplasms). The incidence of foodborne cases been linked to Salmonella infections, especially of nontyphoidal Salmonella gastroenteritis among young children. Unlike nontyphoidal Salmonella serovars, Every year, nontyphoidal Salmonella organ- the enteric fever serovars (Salmonella Typhi, isms are one of the most common causes of Paratyphi A, Paratyphi B [sensu stricto]) are laboratory-confrmed cases of enteric disease restricted to human hosts, in whom they cause reported by the Foodborne Diseases Active clinical and subclinical infections. Infection with enteric fever serovars common nontyphoidal Salmonella serovars, implies ingestion of a food or water vehicle approximately 45% of children younger than contaminated by a chronic carrier or person 5 years excrete organisms, compared with 5% with acute infection. Although typhoid fever of older children and adults; antimicrobial (300�400 cases annually) and paratyphoid therapy can prolong excretion. Approximately fever (~150 cases annually) are uncommon in 1% of adults continue to excrete nontyphoidal the United States, these infections are highly Salmonella organisms for more than 1 year. Consequently, most typhoid fever and paratyphoid fever infections in residents of the United States are usually acquired during international travel. For enteric trimethoprim-sulfamethoxazole is recom- fever, 7 to 14 days (range, 3�60 days). Resistance to these antimicrobial agents is becoming Diagnostic Tests more common, especially in resource-limited Isolation of Salmonella organisms from cul- countries. In areas where ampicillin and tures of stool, blood, urine, bile (including trimethoprim-sulfamethoxazole resistance duodenal fuid�containing bile), and material is common, a fuoroquinolone or azithro- from foci of infection is diagnostic. Once anti- oped, as have commercial immunoassays microbial susceptibility test results are avail- that detect antibodies to antigens of enteric able, ampicillin or cefriaxone for susceptible fever serovars. Multiplex polymerase bacteremia or septicemia, caused by nonty- chain reaction platforms for detection of phoidal Salmonella or for enteric fever caused multiple viral, parasitic, and bacterial patho- by Salmonella Typhi, Paratyphi A, and Para- gens, including Salmonella, have been licensed typhi B, 14 days of therapy is recommended, for diagnostic use. Terapy with a fuoroquinolone marrow, or bile culture is diagnostic because or azithromycin orally can be considered in organisms are ofen absent from stool. The patients with uncomplicated infections for sensitivity of blood culture and bone marrow nontyphoidal Salmonella. For enteric fever culture in children with enteric fever is approx- caused by Salmonella Typhi, therapy should imately 60% and 90%, respectively. For nation of a single blood culture plus culture localized invasive disease (eg, osteomyelitis, of bile (collected from a bile-stained duodenal meningitis), at least 4 to 6 weeks of therapy string) is 90% sensitive in detecting Salmonella is recommended. Drugs of choice, route of Typhi infection in children with clinical administration, and duration of therapy are enteric fever. Multi- Treatment drug-resistant isolates of Salmonella Typhi and Antimicrobial therapy is usually not indicated Paratyphi A (exhibiting resistance to ampicil- for patients with asymptomatic infection or lin, chloramphenicol, and trimethoprim- uncomplicated (noninvasive) gastroenteritis sulfamethoxazole) and strains with decreased caused by nontyphoidal Salmonella serovars susceptibility to fuoroquinolones are common because therapy does not shorten the duration in South and Southeast Asia and are increas- of diarrheal disease and can prolong duration ingly found in travelers to areas with endemic of fecal excretion. Invasive salmonellosis attributable eft, antimicrobial therapy is recommended to strains with decreased fuoroquinolone sus- for gastroenteritis caused by nontyphoidal ceptibility is associated with greater risk for Salmonella serovars in people at increased risk treatment failure. Azithromycin is an efective of invasive disease, including infants younger alternative for people with uncomplicated than 3 months and people with chronic gastro- infections. Chronic car- critically ill patients in whom relief of mani- riage in children is uncommon. The carrier state may be eradicated by 4 weeks of usual regimen is high-dose dexamethasone oral therapy with ciprofoxacin or norfoxacin, given intravenously. High-dose parenteral ampicillin can also be used if 4 weeks of oral fuoroquino- lone therapy is not well tolerated. Salmonella species are gram-negative, aerobic, rod-shaped, zoonotic bacteria that can infect people, birds, reptiles, and other animals. The sale of turtles less than 4 inches in length has been banned in the united States since 1975. The ban by the uS Food and Drug Administration has prevented an estimated 100,000 cases of salmonellosis annually in children. Salmonella ser Typhi, the bacterium responsible for causing typhoid fever, has a preference for the Image 120. Salmonella pathologic changes in brain tissue due to septicemia has been associated with subsequent Salmonella ser Typhi bacteria. Salmonella infection of virtually every organ system, and the septicemia has been associated with subse- nervous system is no exception. Courtesy of quent infection of virtually every organ system, Centers for Disease Control and Prevention/ and the nervous system is no exception. Here Armed Forces institute of Pathology, Charles we see an acute infammatory encephalitis due N. Clinical Manifestations Etiology Scabies is characterized by an intensely pruri- The mite Sarcoptes scabiei subsp hominis is the tic, erythematous, papular eruption caused by cause of scabies. The adult female burrows in burrowing of adult female mites in upper layers the stratum corneum of the skin and lays eggs. In older chil- molt to nymphs and then to adults, which mate dren and adults, the sites of predilection are and produce new eggs. The entire cycle takes interdigital folds, fexor aspects of wrists, exten- approximately 10 to 17 days. S scabiei subsp sor surfaces of elbows, anterior axillary folds, canis, acquired from dogs (with clinical waistline, thighs, navel, genitalia, areolae, mange), can cause a self-limited and mild abdomen, intergluteal clef, and buttocks.
Syndromes
- Eating small amounts of food throughout the day.
- Your doctor or nurse will tell you when to arrive at the hospital.
- Ethyl alcohol
- Urine culture
- Frozen or refrigerated foods that are not stored at the proper temperature or are not reheated the right amount
- Pulmonary function tests (PFTs) to check for any breathing problems
- Speech impairment
- Fainting and lightheadedness
- Commonly used antibiotics include trimethoprim-sulfamethoxazole, amoxicillin, Augmentin, doxycycline, and fluoroquinolones. (Tell your health care provider if you might be pregnant before taking these drugs.)
It descends over the subscapularis 20mg esomeprazole sale gastritis inflammation diet, and reaching its lower border it passes backwards through the quadrangular space described above order esomeprazole 40 mg with mastercard gastritis pain in back, in company with the posterior circumfex humeral artery trusted esomeprazole 20 mg gastritis diet ���. As it passes through the space it is closely related to the capsule of the shoulder joint which lies above it order 40mg esomeprazole overnight delivery gastritis symptoms pdf. The anterior branch passes laterally and forwards round the surgical neck of the humerus and ends by sup- plying the deltoid. The posterior branch supplies the posterior part of the deltoid and also the teres minor. CliniCal Correlation the axillary nerve can be injured in a fracture through the surgical neck of the humerus. In the back and scapular region we see some arteries that begin in the neck as (direct or indirect) branches of the subclavian artery. Like the axillary artery, the subclavian artery is divided into frst, second and third parts (by a muscle called the scalenus anterior). A short artery called the thyrocervical trunk arises from the junction of the frst and second parts of the subcla- vian artery (4. The suprascapular artery descends into the scapular region and is described below. The distribution of the third branch of the thyrocervical trunk is variable, and depending on this, the artery is given alternative names. It divides into a superfcial branch, (which is confned to the neck), and a deep branch which descends into the back in company with the dorsal scapular nerve. In the second variant the third branch of the subclavian artery is called the superfcial cervical artery. This artery supplies the same territory as the superfcial branch of the transverse cervical artery. When this is the case we fnd that the dorsal scapular nerve is accompanied by an artery arising directly from the third part of the subclavian artery: this is the dorsal scapular artery. The superfcial branch of the artery (or, alternatively, the superfcial cervical artery) runs laterally across the posterior triangle of the neck to reach the trapezius. The deep branch of the transverse cervical artery (or the dorsal scapular artery) passes laterally and backwards in the lower part of the posterior triangle of the neck to reach the upper angle of the scapula. It then runs along the medial border of this bone up to the inferior angle: in this part of its course it lies, at frst deep to the levator scapulae, and then deep to the rhomboideus muscles. It gives branches that pass ventral or dorsal to the scapula to anastomose with the suprascapular and sub- scapular arteries. It then passes backwards to reach the superior border of the scapula: here it passes above the transverse scapular ligament and enters the supraspinous fossa. After giving some branches to the supraspinatus it passes into the infraspinous fossa. The suprascapular artery gives off cutaneous branches to the upper part of the chest (suprasternal branch) and to the acromial region (acromial branch). On the back of the body of the scapula the suprascapular artery anastomoses with the deep branch of the trans- verse cervical artery and with the circumfex scapular branch of the subscapular artery (4. On the ventral surface of the body of the scapula, branches of the suprascapular artery anastomose with the subscapular artery and with the deep branch of the transverse cervical artery. Over the acromion branches of the suprascapular artery anastomose with the thoracoacromial and posterior circumfex humeral arteries. It may be noted that the anastomoses around the scapula described above connect the frst part of the subcla- vian artery to the third part of the axillary artery. They serve as collateral channels in case of obstruction to the arterial trunk between these levels. The collaterals take time to become effective and are useful in gradual obstruction of the artery. If the axillary artery has to be ligated the collateral circulation may be inadequate. The upper lateral cutaneous nerves of the arm supply skin over the lower part of the deltoid. The lateral cutaneous nerve of the forearm supplies skin on the lateral aspect of the arm near the cubital fossa (See below). The area of supply of these nerves extends on to the lateral parts of the front and back of the arm also. It supplies skin on the foor of the axilla and then descends into the arm to supply skin on the medial side of the upper part of the arm. The medial cutaneous nerve of the arm is a branch of the medial cord of the bra- chial plexus. It runs downwards frst on the medial side of the axillary vein and then on the medial side of the basilic vein. The medial cutaneous nerve of the forearm supplies the medial aspect of the arm near the cubital fossa (See below). The greater part of the skin on the front of the arm is supplied by the nerves supplying the lateral and medial aspects (as noted above). A broad strip on the front of the arm is supplied by branches of the medial cutaneous nerve of the forearm. On the posterior aspect of the arm also the main supply is by nerves supplying the medial and lateral aspects (named above). Over the middle of the back of the arm a strip of skin is innervated by the posterior cutaneous nerve of the arm (branch of radial nerve), and lower down by the posterior cutaneous nerve of the forearm (branch of radial nerve). Chapter 5 � Cutaneous Nerves and Veins of the Free Upper Lim b 85 Cutaneous Nerves Supplying the Front of the Forearm 1. The lateral cutaneous nerve of the forearm is a continuation of the muscu- locutaneous nerve. The medial cutaneous nerve of the forearm is a branch of the medial cord of the brachial plexus. The nerve runs downwards on the medial side of the axillary artery (between it and the axillary vein), and then on the medial side of the brachial artery. It gives some branches to the skin on the front of the arm and then divides into anterior and posterior branches that run on the corresponding aspects of the medial part of the forearm. The medial and lateral parts of the back of the forearm are supplied by the nerves already seen from the front (medial and lateral cutaneous nerves of the forearm). The greater part of the skin of the back of the forearm is supplied by the posterior cutaneous nerve of the forearm. In front, these are the lateral and medial cutaneous back of the upper extremity nerves of the forearm; and behind there is the posterior cutaneous nerve of the forearm. The greater part of the hand is, however, supplied by cutaneous branches of the median, ulnar and radial nerves. The skin on the palmar aspect of the hand is supplied mainly by branches of the ulnar and median nerves (5.
In the setting of an the tendons can also help to identify the tendon and any infected ?nger discount 20mg esomeprazole amex gastritis symptom of celiac disease, the ultrasound ?nding of ?uid within the surrounding abnormalities (32) generic esomeprazole 20mg visa gastritis symptoms pdf. Imaging pitfalls and limitations References � As in all imaging generic esomeprazole 40 mg mastercard gastritis treatment probiotics, very large patients will be more di?cult 1 discount esomeprazole 40 mg with mastercard antral gastritis diet plan. Radiol Clin North to image, especially when deeper structures such as the hip Am 2002;40:363�86. Legome E, Pancu D: Future application for emergency a portion of the tendon may appear hypoechoic due to ultrasound. Grassi E, Farina A, Filippucci E, Cervinin C: Sonographically forearm fractures in children: a viable alternative? Adhikari S, Marx J, Crum T: Point-of-care ultrasound diagnosis ultrasound: joint sonography. Cusick and Katrina Dean 2 the use of ultrasound in the evaluation of soft tissue struc- accurate. A second study in 2007 suggested that the use of tures has many potential applications. When used judiciously, bedside soft tissue ultrasound may hold a profound impact on soft tissue ultrasound may improve the clinician�s diagnostic management. In those patients believed to be unlikely to have accuracy, result in more appropriate treatment, and improve a ?uid collection requiring drainage, ultrasound changed patient comfort during diagnostic and therapeutic proce- management in 48%. This modality serves as an extension to the clinician�s would require a drainage procedure, emergency ultrasound physical exam and allows real-time visualization during pro- changed management in 73% of this patient group (7). The role for the relative accuracy and potential for profound impact on ultrasound in disease states involving the soft tissues con- patient care nearly mandates the use of bedside ultrasound in tinues to expand with the increased utilization of bedside the patient with an undi?erentiated soft tissue infection. This chapter focuses on In addition to a well-documented role in the di?erentia- three indications well documented in the literature: soft tissue tion of cellulitis and abscess, there have been several reports of infections, foreign bodies, and peritonsillar abscesses. Recently, ultrasound in the diag- Skin and soft tissue infections nosis of necrotizing fasciitis has been described (8). In this single center study of 62 patients with suspected necrotizing fasciitis, the ?ndings of di?use subcutaneous thickening and Indications at least 4 mm of ?uid accumulating along the deep fascial the patient presenting with signs or symptoms consistent layer had good sensitivity and speci?city when compared with with a soft tissue infection requires accurate diagnosis to histologic diagnosis. Clinicians across disci- a woman who presented with clinically suspected necrotizing plines are evaluating an increasing number of soft tissue fasciitis (9). This patient had an ultrasound that showed infections, particularly those associated with community- thickened deep fascia, ?uid tracking, and ?uid pockets mea- acquired methicillin-resistant Staphylococcus aureus (1�4). This ance or protuberant swelling were sought as indicators of caused surgical treatment to be delayed, and the patient suf- a cutaneous abscess. However, the use of ultrasound provides authors have reported the utility of bedside ultrasound in the a noninvasive tool to distinguish between cellulitis and management of perirectal abscesses (16), complicated breast abscess. In certain clinical scenarios, the information abscesses (10), and abscesses of the head and neck (5�17). Incision and superior when compared with incision and drainage as the drainage of a cutaneous abscess can be performed using static gold standard (6). Of the 100 patients enrolled in this study, or dynamic guidance and may prove of particular utility in there were 18 disagreements between clinician impression di?cult cases. Direct visualization of the needle or scalpel 359 and ultrasound ?ndings; in 17 of these cases, ultrasound was entering a ?uid collection may result in increased patient 21:18:18 26 Seric S. Cusick and Katrina Dean comfort and permit avoidance of important surrounding to recognize associated structures, and inadequate patient structures. Maximizing ultrasound system controls and appro- tent ?uid collections, particularly in those of a loculated priate patient preparation and positioning may alleviate many nature. Although the role for bedside ultrasound in the manage- ment of soft tissue infections o?ers many advantages, it is not Imaging considerations without limitations. Certain anatomical locations and patient When evaluating a soft tissue infection with ultrasound, con- conditions may not be amenable to sonographic evaluation, sideration of several key principles will increase the potential despite the measures mentioned previously and genuine for successful image acquisition. In the majority of patients with small, poorly de?ned, subcutaneous ?uid of cases, the use of a high-frequency linear probe (7 to collections detected on ultrasound has yet to be de?ned. In the exceptional case of a particularly deep col- report (8) describes encouraging results for the use of ultra- lection, a curved or phased array probe of lower frequency (3 sound in the assessment of this critical condition. Regardless of the probe used, the sonologist should a primary diagnostic tool for necrotizing fasciitis and imple- attempt to follow the convention of directing the indicator menting a protocol (19). Because of the reliance on di?erences in echogenicity for accurate image interpretation, the ultra- Soft tissue foreign bodies sound should be performed in a dim room, a?ording the use of minimal total gain. Appropriate use of image depth will Indications improve visualization of the structures of interest, maximize Soft tissue foreign bodies represent a troubling entity for frame rate, and allow accurate assessment of tissue involve- emergency physicians. They often pose remarkable clinical ment and the intended depth of any procedure to follow. The traditional approach to these painful or super?cial infections � such as the hand � the use of patients has often included a combination of plain radiogra- a commercially available stando? pad or water bath may be phy and local wound exploration at the bedside. However, used to improve patient tolerance and enhance image quality wound exploration has potential disadvantages, including by minimizing the e?ect of the near-?eld acoustic dead space patient discomfort, damage to nearby structures, and (18). Alternatively, a latex glove ?lled with water or a 250-cc increased possibility of infection. Application of bedside ultrasound may facilitate surrounding (or contralateral) normal tissue to appreciate the e?cient diagnosis and appropriate management of these normal tissue planes and associated anatomical structures. The a?ected area is then evaluated in orthogonal planes, observing changes in echogenicity of the subcutaneous tis- Diagnostic capabilities sues, the presence of edema, and the location and size of any In evaluating the use of ultrasound in the detection of foreign ?uid collections. Cellulitis is characterized by an increased bodies, one must consider the other imaging modalities avail- thickness of the subcutaneous layer that is relatively hyper- able. Plain radiography has excellent sensitivity for metallic, echoic compared to normal tissue. As the infection � and glass, and mineral-based foreign bodies but variable � and associated swelling � increases, hyperechoic fat globules are generally poor � sensitivity for wooden, plastic, and organic outlined in hypoechoic edema, yielding the appearance materials. Both of these cross-sectional as spherical and anechoic to hypoechoic, often containing imaging modalities a?ord precise localization of foreign echogenic debris. However, atypical ?uid collections may be bodies in relation to adjacent anatomical structures and may near isoechoic and have complex loculations and septations. Peterson and Imaging pitfalls and limitations colleagues found that the best modality for detecting retained 360 Common pitfalls in scanning soft tissue infections include wooden foreign bodies is ultrasound, although it is frequently improper probe selection, poor use of depth and gain, failure underused (27). Vascular structures may be and has been reported across several disciplines (28�32). The majority of these objects will be tissue models and clinical investigations, ultrasound appears hyperechoic and associated with artifacts cast into the far accurate. Metallic objects are hyperechoic and may cause rever- ultrasound to have sensitivities of 95. Wood and mineral-based foreign bodies (rock, series evaluating ultrasound in the detection of wooden for- gravel) are often brightly re?ective with dense posterior sha- eign bodies of the hand and foot, the sensitivity was 95% to dowing. Plastic and rubber are similarly hyperechoic with 100%, and particles as small as 2 mm were visualized with variable posterior shadowing, although plastic may, on occa- ultrasound (29, 30). As the local tissue reaction develops, the foreign the absence of clinical ?ndings and an associated in?amma- body will develop a characteristic hypoechoic halo (43) indi- tory reaction may be partly responsible for the low sensitiv- cative of the surrounding in?ammation and edema. Despite its Ultrasound-guided removal of foreign bodies allows esti- promised utility, further prospective evaluation of emergency mation of the object�s depth and proximity to anatomical physician-performed ultrasound for foreign body detection is structures. Static � or indirect � guidance permits identi?ca- needed to characterize the accuracy of this modality.
The white lines in this ?gure show the two air-?uid levels in the same loop of bowel order esomeprazole 40mg on line gastritis weight gain. The black lines in this ?gure show the two air-?uid levels in the another loop of bowel order esomeprazole 40mg overnight delivery gastritis vs gerd. It may be helpful to think of this image when considering a small bowel obstruction order 20 mg esomeprazole with visa gastritis upper right back pain. The term �malrota- this diagnosis as soon as possible and to arrange for tion� places emphasis on the embryology of this immediate surgical reduction to restore bowel perfusion buy 40 mg esomeprazole otc xyrem gastritis. This a stalk� syndrome to refocus attention on the clinical con- compression can also result in a high bowel obstruction. Guts on a stalk are prone to However, this does not compromise blood ?ow, and it is not twisting as a midgut volvulus (illustrated in Fig. A midgut volvulus is potentially catastrophic and is a true Patients born with a malrotation (guts on a stalk) are likely 148 surgical emergency. The midgut volvulus involves the entire to sustain a midgut volvulus at some point in their lives. The popcorn-like appearance is preserved so that, in most instances, the bowel is not distended. In some areas, the bowel diameter is large, but this is not the criterion to determine bowel distention in children. Bowel distention is con?rmed when the bowel walls are smooth (like hoses and sausages). Air-?uid levels: many air-?uid levels, but note that they are all small and none can be clearly identi?ed to be in the same bowel loop (no J-turn or candy cane phenomenon). Roughly 50% of malrotation patients will present with Diagnosing midgut volvulus is much more di?cult in older a midgut volvulus in the neonatal period. Coupled with a history of bilious vomiting, a gasless 150 diately suspected in any neonate with bilious vomiting. One of the concerns with newborns, neonates, or very young infants is that they might have a congenital malformation that has yet to reveal itself. The left image is a ?at view, whereas the right image has contrast in the lower bowel. There are four large bubbles of gas, and the rest of the abdomen is fairly gasless. This should be regarded as a poor gas distribution, suggesting a bowel obstruction. Considering the large gas collection on the right is unlikely to be the stomach, it is too large to be normal nondistended bowel. This clearly does not resemble popcorn or sausages, but it is orderly and not random or disorderly. The contrast enema on the right shows a microcolon indicating the absence of bowel contents passing to the colon during gestation. The presence of a microcolon suggests that the distal small bowel is also atretic. Most of the gas is trapped in of time to feed, excrete stool, and form normal amounts of gas the stomach, suggesting a high bowel obstruction. Although intussus- 152 because this infant had been doing well for 3 months (plenty ception might also be possible, it generally obstructs in the 10:32:23 09 Chapter 9: Plain Film Radiographs of the Pediatric Abdomen Figure 9. The dilated stomach seen here suggests a high obstruction, such as a midgut volvulus. Note the corkscrew appearance of the small bowel as the barium exits the stomach (black arrow). If the gastric contrast is unable to exit the stomach, the Thin contrast such as thin barium or water-soluble contrast is image will result in an abrupt halt of the advancing contrast. As the volvulus initiates its ?rst twist, there is roughly an even chance of twisting further (getting tighter) or untwisting itself. This twisting and untwisting result in �intermittent volvulus,� which presents with pain and vomiting that resolves on its own. Patients with such a history should be imaged to determine if they have a malrotation that is intermittently twisting. When a patient presents with severe acute symptoms, an imaging strategy should focus on con?rming the presence of a midgut volvulus. However, if the patient is well on presenta- tion but gives a history of intermittent symptoms that suggest the possibility of an intermittent volvulus, then the imaging strategy should focus on con?rming the presence of Figure 9. It is suspended on the left by the ligament is a later decubitus view because the patient was too ill to stand. A contrast enema can the lateral decubitus view demonstrates some air-?uid level in potentially identify a malrotation if the cecum is misplaced. This patient�s past history ?oating and just happens to be in the correct location when is interesting in that she had periodically complained of inter- the contrast enema is performed, it will fail to identify the mittent abdominal pain, as well as vomiting and dehydration malrotation. In a patient with a malrotation, the midgut could a malrotation by examining the vascular supply of the bowel. This radiographic sign is uncommon in acute appendicitis, Appendicitis but when it is present, it is highly suggestive of acute appendicitis. Roughly half of the patients with will encounter only a few appendicoliths in their career. This case shows an x-ray of the appendix specimen that patient�s left (right on image), but note that this is not the case on was removed at appendectomy. Look at the peritoneal fat stripe on narrow space between the fat stripe and the bowel. The bowel should generally lie very the patient�s right, the bowel is farther away from the fat stripe, 156 close to this fat stripe (white arrows), which is what is seen on the suggesting that there is ?uid, a mass, or thickened tissue pushing 10:32:23 09 Chapter 9: Plain Film Radiographs of the Pediatric Abdomen Figure 9. There is a small gas pocket that does not appear with intussusception will have normal abdominal radio- to be within the bowel (black arrow). It is generally not possible to rule out intussusception highly suggestive of a ruptured appendix. Most cases of intussusception occur in infants, but toddlers As a brief summary, the radiograph signs of intussuscep- can be a?ected as well. Intussusception most often occurs in tion are the target sign, the crescent sign, absence of the the ileocecal region. If the direction of the crescent is the target sign is always found in the right upper quadrant reversed, it is more likely that this is not a true crescent sign. If the crescent sign is identi?ed, the likelihood of intussuscep- It resembles a donut with the center hole still ?lled in. To identify the target sign, one must search Other signs of intussusception are the absence of the for it. If the gas pocket is large, the shape might not look like will become more edematous, thus obliterating the normal a crescent sign. This should more accurately be called the interface of the liver edge with non-gas-?lled bowel. This is �intussusceptum protruding into a gas-?lled pocket sign,� a less speci?c sign of intussusception.
Discount esomeprazole 40mg fast delivery. డా . ఖాదర్ గారి కాషాయాల PDF Book || Download Dr Khadar vali PDF Book Telugu | Dr Khadar vali telugu.