
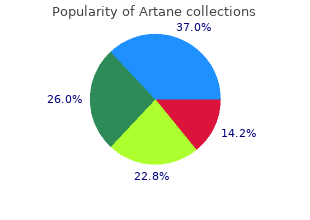
Lancaster Theological Seminary. N. Mufassa, MD: "Buy online Artane - Proven Artane online".
Conduction Defects in Patients with Atrial Fibrillation and Flutter Many patients with atrial fibrillation and macroreentrant purchase 2 mg artane visa stomach pain treatment natural, tricuspid-caval isthmus-dependent atrial tachycardia (i generic 2mg artane free shipping laser treatment for dogs back pain. These are characteristic findings of so-1 called left atrial abnormality and are present in the vast majority of patients with atrial flutter or fibrillation purchase 2 mg artane with mastercard pain hypersensitivity treatment, regardless of the underlying etiology discount 2 mg artane overnight delivery pain treatment wellness center. The broad notched P wave in the inferior leads is the most common abnormality, while the exaggerated negative terminal force in V is the next most common. One or more of these1 abnormalities are seen in 80% to 85% of patients with these arrhythmias. In nearly two-thirds of patients, the P-wave duration exceeds 120 msec when all 12 leads are assessed simultaneously. For patients with so-called left atrial abnormalities, right atrial conduction time is normal in 80% of patients with a mean right atrial conduction time of less than 50 msec. For the remaining patients, right atrial conduction time was only modestly prolonged except for six patients with dilated cardiomyopathy who had prolonged right atrial conduction times exceeding 62 msec. Where the site of delay is located is unclear, but there appears to be delay between the right and left atrium at the region of Bachmann bundle as well as at the lower septum. A more detailed analysis of intra-atrial conduction during sinus rhythm in patients with atrial fibrillation is important to assess the potential role, if any, of intra-atrial conduction disturbances in the pathogenesis of atrial fibrillation. Detailed mapping with the Carto system (Biosense, Cordis/Johnson and Johnson, see Chapter 3) has been of value in this regard. Correct interpretation of intra-atrial and interatrial conduction requires mapping along the posterior left atrium and left atrial septum in order to more specifically localize the sites of delay. They have quantified them in terms of duration and number of fragmented deflections as defined by the number of negative deflections in the electrogram. Abnormal electrograms were defined as those with a duration of ≥100 msec and/or eight or more fragmented deflections. Twelve atrial sites, including anterior, lateral, posterior, and septal sites were measured at the high-, mid-, and low-right atrium. Only 23% of control patients had any fractionated electrograms while 68% of patients with paroxysmal, lone atrial fibrillation and 83% of patients with atrial fibrillation/flutter and sick sinus syndrome had abnormal electrograms. The absence of any left atrial mapping data limited the ability to establish a causal relationship of these abnormal electrograms to the presence of atrial flutter or fibrillation. These electrograms, however, do represent marked nonuniform anisotropy and suggest an increased amount of fibrosis in those patients with these electrograms and atrial fibrillation. Whether these abnormalities are casually related to atrial fibrillation is unknown, but they may represent a potential substrate under specific circumstances. We and others have been interested in evaluating the response of intra-atrial conduction to atrial extrastimuli 9 10 11 12 9 during atrial pacing at cycle lengths of 600 and 450 msec. No conduction delays were noted in response to late coupled extrastimuli in both control patients and those with atrial fibrillation or flutter. However, as extrastimuli were delivered with increasing prematurity, progressive intra-atrial conduction delay occurred. In patients without a prior history of arrhythmias (controls), intra-atrial conduction delays only occurred at coupling intervals just above refractoriness, whereas in those patients with a history of atrial flutter and or fibrillation, conduction delays occurred at much longer coupling intervals (Figs. The differences in response to atrial extrastimuli between control patients and those with atrial flutter or fibrillation are shown in Figures 9-3 and 9-4. While in the control patients there was very little conduction delay up to atrial refractoriness, in patients with a prior history of typical tricuspid-caval isthmus- dependent atrial flutter of fibrillation these atrial conduction delays were seen beginning 50 msec above refractoriness. There are no data available in patients with other macroreentrant atrial tachycardias, although the association with atrial fibrillation suggests they would respond similarly. Of note, when atrial extrastimuli were delivered at a paced cycle length of 450 msec, there was no difference in maximum conduction delay between control patients and those with atrial flutter and fibrillation. This was related to the ability of the control group to achieve shorter coupling intervals, and maladaptation of refractoriness noted in patients with a history of atrial flutter and fibrillation (see subsequent paragraphs). These data, however, suggested that a greater degree of intra-atrial conduction delay in response to relatively late atrial extrastimuli might be a marker for those patients 9 12 predisposed to atrial arrhythmias. S -S represents coupling intervals of extrastimuli to the last beat of an1 2 eight-beat drive at paced cycle lengths of 600 msec for each patient. Stimulation in each patient was performed at the right atrial appendage at a drive cycle length of 600 msec. Progressively premature extrastimuli only produce slight intra-atrial conduction delays of 20 to 25 msec at coupling intervals just above atrial refractoriness. Progressive intra-atrial conduction delay occurs in response to increasing prematurity of extrastimuli. Second, in those patients in whom atrial fibrillation was induced, a greater degree of delay was noted in the triangle of Koch than in those patients in whom no atrial fibrillation was induced. Third, the local electrogram duration in the posterior triangle of Koch was longer in those patients who developed atrial fibrillation in response to atrial stimulation than in those who did not (Fig. These data suggest the prolonged conduction times during high-right atrial stimulation are common to patients with palpitations regardless of whether or not atrial fibrillation is inducible. However, nonuniform anisotropy in the area of the posterior triangle of Koch, and perhaps elsewhere, is quite important since left atrial extrastimuli rarely induce atrial fibrillation or flutter and are rarely associated with intra-atrial conduction delay, particularly in the posterior triangle of Koch (Fig. Additional studies using high-density mapping in both atrial chambers would be critical to decide if any particular site of conduction delay is necessary for initiation of atrial fibrillation and/or flutter. Such studies suggest that the crista forms a functional arc of block in most cases. During slow pacing from these areas, no split potentials are usually seen; however, during rapid pacing from the low posterior right atrium split potentials with opposite activation sequences are 20 21 23 seen. The opposite activation sequence reflects activation caudocranially from the posterior to the crista terminalis and craniocaudally lateral to the crista terminalis. The longest cycle length at which transverse cristal 20 block appeared was increased slightly by propranolol and to a greater extent by procainamide. They suggested that this is the reason that counterclockwise flutter is more frequent than clockwise flutter. However, other factors must be involved since counterclockwise flutter is also induced in transplanted hearts in which the crista 24 terminalis cannot play a role. We have recently evaluated the presence and degree of anisotropy on intra-atrial conduction velocity measured from a high-density (240 poles; 2. Intra-atrial conduction velocity was measured in 16 radii during pacing from the center of the plaque at 600 msec, the fastest rate of 1:1 conduction (F max), and at a rate just above local atrial refractoriness. We found no differences in the degree of anisotropy in patients with chronic atrial P. This reduction was specifically related to a decrease in conduction velocity parallel to fiber orientation (in the so-called rapidly conducting direction) (Table 9-1). All patients showed significant direction-dependent conduction (anisotropy) with the fastest conduction perpendicular to the A-V groove (Fig. The relationship to this pattern of conduction to the activation patterns during atrial fibrillation will be discussed subsequently. In the diagrams, pacing is delivered medial to the potential barrier of the crista terminalis.
For various reasons discussed earlier in this chapter generic artane 2mg amex midwest pain treatment center fremont ohio, I do not believe the fascicles have been proven to be part of the reentrant circuit cheap 2mg artane free shipping pain medication for dogs post surgery. These tachycardias frequently demonstrate 345 diastolic potentials on the septum leading to a zone of slow conduction buy 2mg artane with mastercard pain treatment and wellness center greensburg pa, but such potentials have not been universally found 2mg artane sale best pain medication for a uti. The widely separate potentials are recorded from opposite sides of the ventriculotomy scar. Electrophysiologic characteristics of sustained ventricular tachycardia occurring after repair of tetralogy of Fallot. The mode of initiation, response to stimulation, and effect of drugs on such tachycardias will also provide indirect evidence for the type of mechanism for the arrhythmia. Of importance, however, is the recognition that because tachycardias in cardiomyopathy may be midmyocardial or even subepicardial, the earliest site of activation on the endocardium P. This is important because most standard radiofrequency catheter ablation techniques result in a lesion <2 to 5 mm in depth and could therefore fail to ablate a tachycardia that is subepicardial. Epicardial mapping or use of newer technologies may be necessary to define critical sites for ablation in patients with nonreentrant mechanisms and/or cardiomyopathies in whom intramural or subepicardial sites are critical. The ablation catheter is recording from sites A, B, and C on the schema at the top with recordings shown in the panels on the bottom. This occurs because many potential channels can go through the scar leading to many different tachycardia circuits. In the remaining 15% of 368 369 370 tachycardias, reentrant circuits and/or exit sites are more disparate. In the presence of coronary artery disease, the vast majority of all tachycardias, regardless of morphology, arise in or near the subendocardial surface of the left ventricle. C: A tachycardia with a right bundle branch block, right inferior axis pattern is seen. This site is 2 cm above site 3 and forms the 2 apex of a triangle between three sites, which cover an area of approximately 3. Although individual tachycardia morphologies can be initiated at different times, not infrequently one tachycardia changes to another in response to programmed stimulation (Fig. In such cases, we believe that stimulation either causes a change in location or direction of activation from the site of exit from the reentrant circuit or a change in the activation sequence in the ventricular tissue surrounding the exit site by altering the electrophysiologic properties of this tissue. Occasionally, the change in configuration is abrupt, suggesting a change in exit pattern (Fig. In either of the latter two instances, because the reentrant circuit is unaffected, the tachycardia cycle length is unaffected as well. Thus, change in tachycardia morphology need not reflect a change in a reentrant circuit or site of impulse formation but merely reflects the overall pattern of ventricular activation. The cycle length may also be altered because the conduction velocity through nonuniform anisotropic tissue can change based on the direction of the 404 propagating wavefront. Changes in cycle length, sites of origin, or direction of the propagating wavefront can result in failure to propagate to or through other areas of the ventricle that are not necessary for the maintenance of the tachycardia. An example is shown in Figure 11-254; an area of a left ventricular aneurysm is activated by every cycle of a tachycardia with a cycle length of 350 msec but suddenly fails to be activated during every other complex of a new tachycardia with a shorter cycle length. In other instances, a larger macroreentrant figure-of-eight reentrant pathway has been 46 352 353 371 374 375 376 described. A bipolar catheter is schematically positioned over part of the reentrant circuit and records a local fragmented activity during different parts of the cardiac cycle, depending on the relationship of the exiting wavefront to the catheter recording site. However, the successful outcome of a catheter ablation to define the accuracy of mapping is often unjustified because multiple radiofrequency applications at different sites are frequently used, prohibiting analysis of the importance of any single local electrogram. Use of the postpacing 405 interval alone is inadequate, but contrary to the suggestion of Bogun et al. Obviously, thickness of scar, presence of endocardial clot, a wide isthmus or no isthmus (single loop reentry), intramural or subepicardial location, and inadequate lesion make 100% success an unrealistic goal. This suggests that a change in exit site has occurred in the absence of any change in the underlying tachycardia mechanism. On cessation of pacing, the tachycardia morphology has reversed itself to a left bundle branch block pattern. This suggests that overdrive pacing stopped the tachycardia and reinitiated in the opposite direction. We have performed both catheter and intraoperative maps on several hundred tachycardias to date and have found an excellent correlation between the catheter map and the intraoperative map. Early intervention of acute infarction may change this; however, I believe the change in substrate is more likely to change the type of tachycardia to one that is more unstable. Mapping such tachycardias will require the use of newer technologies as suggested earlier in the chapter. The activation times obtained during catheter mapping closely correspond to data obtained intraoperatively. Role of catheter mapping in the preoperative evaluation of ventricular tachycardia. In such instances, potential arrhythmogenic areas can be identified in the presence of abnormal and/or late electrograms, which we and others have demonstrated to be associated with 31 32 33 34 35 36 38 39 61 arrhythmogenic tissue. Unfortunately, abnormal, fractionated, and/or late electrograms are found throughout infarcted myocardium and are nonspecific 31 385 for the site of origin or critical isthmus. This is also true in patients with right ventricular dysplasia, another disorder in which abnormal electrograms are widespread yet tachycardias have a relatively focal isthmus (Fig. An example of such maps and the relationship of abnormalities recorded during sinus rhythm to the site of successful ablation at an entrainment map defined protected isthmus is shown in Figure 11-260. Some investigators suggest homogenization of the endocardial and epicardial area 406 of low-voltage and abnormal electrograms (see Chapter 13 for discussion). In view of the limitations of voltage mapping related to catheter electrode size and orientation as well as the effects of the wavefront of activation described earlier, this approach clearly destroys tissue that does not need destruction and may miss tissue that does. Comparison of endocardial catheter mapping with intraoperative mapping of ventricular tachycardia. During the tachycardia, the earliest ventricular activation breaks through at the apex of the right ventricle. Currently, there is no way to identify which normal sites are potentially arrhythmogenic; however, evaluating the response of such electrograms to ventricular pacing and extrastimuli might provide some insight into this question (Fig. Further work is necessary to see whether this would be of predictive value and hence can be used clinically. During sinus rhythm, eight sites demonstrate abnormal (A), fractionated (F), or late (L) electrical activity. The value of catheter mapping during sinus rhythm to localize site of origin of ventricular tachycardia. In addition, we studied the 12-lead electrocardiograms produced by pacing of 393 multiple ventricular sites in patients with and without wall motion abnormalities. Furthermore bipolar pacing stimulates an area of ≈1 cm , further limiting the accuracy of this technique. In the presence of infarction this limitation is exaggerated since high currents are often used.
It is therefore important to carefully follow the course of the heal- ing process in order to precociously diagnose a problem and to limit its evolution safe 2mg artane pain treatment gout. It is frequent to observe irritative (contact) or allergic dermatitis generic artane 2mg with amex pain treatment center bismarck nd, formation of milia buy 2 mg artane visa pain treatment center colorado springs co, acne reacutization discount artane 2 mg free shipping pain treatment and wellness center pittsburgh, and postinflammatory hyperpigmentations. Most severe complications, which luckily are rare, involve pathological scarring, ectropion, and disseminated infections. A delayed diagnosis can determine the formation of keloids, permanent depigmentation, and skin necrosis. Pearls and Pitfalls When a laser resurfacing treatment is performed for the first time, prudence guides us to use conservative flu- ences, proceeding gradually to the removal of epidermal layers, until an evident contraction is seen, which identi- fies the reaching of the desired dermal level. First of all, we often • When isolated areas of the face are treated, the entire have a patient under local anesthesia or sedation; as such, a cosmetic unit should be treated. Secondly, it • Do not treat the canthal regions and the upper eyelid is useful to perform a first test on a “safe” area of the face tarsus. After realizing the second and in case the third pas- sage, we should decide when to stop recognizing also Finally, rigorous criteria of patient selection should visually our “end point. T o day, with the aim of being formally informed about the possible risks of the surgical procedure that I wish to undergo, I have been given this consent, which I will return completely filled-in the day of surgery. The laser method allows to reach such target with several advantages: higher precision of action on the damaged skin layers, absence or minimal presence of bleeding, better post-operative course. The most commonly used laser is the Erbium Yag because it is more selective towards the skin: it emits a light beam that heats and vaporizes the skin, reaching the damaged layers with elevated selectivity. In many cases wrinkles appear in localized areas (eye contour, mouth) and the laser can be specifically used on these regions. Patients with olive, tanned or dark skin are at risk for pigmentation abnormalities, as such an attentive evaluation and a spe- cific skin preparation should be performed whenever you decide to undergo the procedure. Patients that have assumed Accutane (isotretinoin) during the last 12 months or that are prone to pathological scarring (i. The procedure of “Laser Skin Resurfacing” can improve the aspect of the face reducing the wrinkles, but only the static ones, while it cannot eliminate the dynamic wrinkles that depend on the mimical movements of the face and that require other surgical procedures to be treated. The procedure always requires an adequate skin preparation for at least three to four weeks and consists of the daily applica- tion of specific products. In case isolated areas of the face are treated local anesthesia is sufficient, while for the treatment of the entire face an intra- venous sedation or general anesthesia will be added. Swelling is always present and its entity depends on both patient’s personal reactivity and depth of treatment, but it is usually reversible during the first 7/15 days. U sually the skin is decisively redden on the first 5/6 days to then become dark pink after the first week and a lighter pink after the second week, until the reddening disappears within one or two months. In special cases and in delicate areas like the eyelids the reddening can last longer and require special treatments in order to fasten the process of normalization of the erythema. From the seventh day on usually most patients can apply a specific covering make-up. It is very important during the following three months to avoid sun exposure until the whole skin color is back to its normal aspect and to use a total block sun protection in any case. The achievement of an optimal aesthetic outcome can require several months, which are necessary for the production of col- lagen, however, when the reddening fades away the patient is already able to notice an evident improvement of skin quality. Despite the high degree of precision of the laser, not all the wrinkles or skin irregularities can be solved with one treatment and in many cases several treatments are needed in order to reach the desired results. It is important to know that the obtained result is not permanent because the new skin will not be unaffected by the aging processes. There is also the possibility of delayed skin healing processes, with the presence of pathological scars and areas of irrevers- ible hypopigmentation, usually due to an excessive depth of treatment. I give consent to be photographed before, during and after surgery with the aim of clinical documentation and possible sci- entific use. Perego Believing of having received clear and precise information on every detail of the surgical procedure I wish to undergo, I undersigned: S urname…………. A n d his co-workers to perform the surgical procedure of:… U n der anesthesia…………in date………………………….. Patient’s signature………………………………………… (or legally authorized representative) S urgeon’s signature……………………………………….. Despite not being considered as part The exploitable fluence varies from 3 to 90 J/cm2. The of the laser family (given the non-collimated and non-coherent spot, which corresponds to the size of the crystal in contact nature of their emission) they have proved their efficacy in with the skin, usually of a rectangular shape, is 10–50 mm interacting with tissues and are still subject to careful and long. Over the patient’s characteristics and of the lesion to be treated in years a number of innovations followed, which allowed to order to avoid complications and adverse effects. Various manufacturers offer different filters as unsuited to light source treatment. The wavelength can be mod- 2 Treatment ulated according to the depth of the targeted tissue; longer waves consent a deeper penetration into the dermis [41 ]. Energy can be conveyed into a single pulse or whether performing skin rejuvenation, epilation, or vascular multiple pulses with delay times of 1–500 ms. A written consent form will be presented, to be read by the patient and possibly M. It is always Dipartimento di Chirurgia , Università di Roma advisable to take photos to document the pretreatment “Sapienza”, Policlinico Umberto I, Rome , Italy e-mail: mariagiuseppina. A test spot will be done in an inconspicuous thema, associated or not with rosacea may appear (Figs. Of course, treatment must necessarily anesthetic creams 20 min in advance may be useful with be preceded by dermatological examination in order to hypersensitive patients. The size and the maneuverability of the handpiece are of crucial importance in the facial treatment, especially on irregular surfaces, like the nose dorsum or the upper lip. Commonly, one pass is sufficient to treat the selected area; however, if required, it is possible to deliver more passes with a different orientation of the handpiece. At the end of the treatment, an erythematous reaction develops, which lasts 2–48 h. To minimize this reaction, zinc oxide ointments are generally used right after or in the fol- lowing hours [37 ]. More sessions are usually necessary according to the pathology to treat, at intervals of 3–4 weeks. The great flexibility of this tech- nique allows simultaneous intervention on all the marks of photoaging [1, 11–13 ] (Fig. This pathology is due to the combined action of two groups of concomitant factors: intrinsic ones (age, genetic disposition, phototype, etc. C l a ssically, a photo-damaged skin shows alterations in skin texture, mainly depletion of the dermis and dehydra- tion. Normally treatment is followed by the appearance of a diffuse erythema and a gradual darkening of hyperpigmentations, which may increase in the next days, to resolve spontaneously in exfoliation of the area.
Syndromes
- Defects in the hemoglobin molecules inside red blood cells
- Swelling, generalized
- Chest CT scan
- Heat the end of the paper clip over an open flame until it is red hot. Use a pair of pliers to hold the paper clip. While it is still very hot, touch the tip of the paper clip to the injured fingernail. Touch the nail over where the blood is collected. This is not a painful procedure for most people.The heat of the clip will burn a small hole in the fingernail. It is not necessary to press hard on the fingernail to burn the hole.
- Legg-Calve-Perthes disease (in boys 4 to 10 years old)
- Sinus pressure
- Complete blood count (CBC) to check for anemia
- Various anti-rust products
- Skin creams to treat burns
New muscle weakness of a mild to moderate motor neuron loss (which can be confrmed through a degree responds well to a nonfatiguing exercise program typical patient history cheap 2mg artane with visa nerve pain treatment options, a neurologic examination 2mg artane mastercard pain treatment center baton rouge louisiana, and order 2mg artane fast delivery drug treatment for shingles pain, and pacing of activity buy cheap artane 2 mg on line key pain management treatment center, with rest periods to avoid muscle if needed, an electrodiagnostic examination). Generalized fatigue may be treated with energy A period of neurologic recovery followed by an interval conservation, weight loss programs and lower extremity (usually 15 years or more) of neurologic and functional orthoses. All cases labeled as dis- 333 muscle fatigue (decreased endurance), muscle atrophy, carded, not polio require thorough justifcation and or generalized fatigue. Exclusion of medical, orthopedic and neurologic con- Indicators of Quality ditions that may be causing the symptoms mentioned above. Many patients require revision of orthotic devices such as braces, canes and crutches or may use new, lighter ortho- Role tic devices to treat new symptoms. Common issues include To identify high-risk areas or groups where polio virus genu recurvatum, knee pain, back pain, degenerative transmission is occurring or is likely to occur. Surgery for scoliosis or fractures To monitor progress so as to determine whether strate- may also be necessary to treat new conditions. For Mopping up denotes the fnal strategy when door to more details, refer See Chapter 28 (Pediatric Neurology). Te encephalitis, etc) cases require to be reported so that there spread is by direct or indirect contact with respiratory is no chance of missing any case of polio. Period of infec- Special Features tivity extends from 24–48 hours before appearance of rash Reverse cold chain: Stool samples (two, at least 24 until formation of scabs (crusts) which are noninfectious. It shows some seasonal to be poliovirus, for fnding whether it is a natural wild variation, the peak incidence being during winter and virus or vaccine-related virus. Outbreak response eforts: Tese should be initiated Te peak age of incidence is 5–10 years, though the promptly without waiting for the stool culture reports disease may occur at any age including neonatal period, 334 adolescence and adulthood, when it frequently takes a Congenital varicella syndrome (varicella serious turn. Stigmata z Skin Cicatrix presenting as a zig-zag scarring in a Clinical Features dermatomal distribution; hypopigmentation. Incubation period is around 15 days, the range being z Brain Aplasia, microcephaly, hydrocephaly and 11–21 days. Te eruption z Eye Microphthalmia, cataracts, optic atrophy and passes through all the stages encountered in smallpox, choreoretinitis. Te Hemorrhagic, neonatal and even congenital chicken- complete evolution takes about 4–7 days followed by scab pox may infrequently be seen. Te scabs (crusts) fall of within 2 weeks of frst chickenpox between 5 days before and 5 days after delivery, appearance of rash. Maternal infection may damage the fetus, Skin lesions of chickenpox appear in 2–4 crops so that causing embryopathy with limb atrophy, scarring of skin, all stages and sizes may be seen at the same time. Further- malformations in relation to extremities and ophthalmic more, these are superfcial, pleomorphic and centripetal (cataracts) and meningeal and brain lesions (calcifcations, in distribution and are seen over the scalp and mucus sur- aplasia), the so-called congenital varicella syndrome faces (including conjunctiva) frst and then over the body. Te trunk is profusely covered whereas extremities and Diagnosis face are only scantly involved. Te disease had got to be difer- On an average, around 10–500 (with a median of 300) entiated from smallpox in by gone era. Early in disease, the pleomorphic lesions are encountered in an individual papules of chickenpox may need to be diferentiated from subject. Chickenpox lesion on healing leave behind pyoderma, insect bite, papular urticaria, drug reaction, macules (hypo or hyperpigmented) for a week or more but, herpes simplex, hand-foot-mouth disease and rarely, eventually, without scar unless secondary infection occurs. Occasionally in children under 2 years of age, chickenpox Laboratory diagnosis is difcult. Itching is lesions, multinucleated giant cells containing intranuclear inclusions and immunoglobulin M (IgM) antibodies may mild at frst, but may become severe in the pustular stage. Te so- called progressive varicella syndrome is a very serious condition characterized by nonstop eruption of varicella lesions which have a tendency to become hemorrhagic secondary to a coagulopathy and multiorgan involvement in the form of hepatitis, pneumonia and encephalitis. Note the pleomorphic centripetal lesions in a usually occurs in immunocompromised states, neonates, 10-year-old patient. Te vaccine is quite safe and z Glomerulonephritis z Hepatitis well tolerated but expensive. Probably susceptible pregnant women exposed to vari- Treatment cella, especially if antibody testing turns out to be nega- tive. Aspirin, however, chickenpox at least until 6 days of appearance of the rash needs to be avoided since it may enhance the risk of to safeguard against an epidemic. Itching may be relieved by systemic antihistaminics Prognosis and/or local application of calamine lotion, potassium Chickenpox carries, as a rule, favorable prognosis. It is the most common and the most infectious of the viral Steroids are, as a rule, contraindicated. It is characterized by catarrhal symptoms followed Children sufering from chickenpox must be restrained by a typical rash, the so-called measly rash. In healthy children, it Acyclovir (Zovirax) claims to accelerate rate of clinical generally runs a more or less benign course. Te peak incidence evidence becomes available for its utility in routine in the developing world is in the age group 1–5 years. One cases of chickenpox, its administration should be attack confers nearly lifelong immunity. Transmission is by indirect or direct contact and droplet infection, portal of entry being respiratory tract. Te period of infectivity is 4 days prior to and 5 days after the appearance of the rash. Pathological changes are essentially limited to superfcial blood vessels of skin and mucus membrane, forming the so-called inclusion bodies. Te infection is highly contagious with secondary attack rates as high as over 90% in susceptible (unimmunized) household contacts. Either no medicines or the ones which are supposed to cause greater eruption are preferred by the folklore. Harm- ful practices such as fomentation with hot bricks, instilling cow milk drops in nostrils and eyes, and giving a purge in order to bring the rash out fully are common. Clinical Features Te average incubation period is 11 days, the variation being between 10 days and 12 days provided that onset is ascribed to the frst prodromal symptoms. Prodromal (Catarrhal) phase of 3–5 days is characterized by upper respiratory catarrh (rhinorrhea, dry cough), fever, malaise, conjunctival congestion and photophobia. Teir frst appearance, usually on second or third day, is over the buccal mucosa, opposite the frst or second lower molar, and then at other sites in the mouth. With the appearance of rash, fever tends to observed in only a small proportion of cases. Even 10–20 days after the onset, complement-fxation antibodies in meaningful titer may be detected. Differential Diagnosis At times, another supposedly viral infection of infant and toddlers, roseola infantum (roseola subitum, ffth disease), may be confused with measles. Te pink macular rash of this infection usually appears on trunk, neck and proximal areas of the extremities only.
Artane 2 mg visa. 10 Exercises & Tips for Knee Pain Relief by Physical Therapy.