
Louisiana State University at Shreveport. I. Topork, MD: "Buy online Female Viagra - Proven Female Viagra online no RX".
Any views expressed by named authors are solely the responsibility of those authors female viagra 100 mg generic women's health clinic denton tx. To reduce that burden an integrated approach is required cheap 50 mg female viagra mastercard women's health 101 running tips, combining health promotion female viagra 50 mg mastercard womens health group brunswick ga, disease prevention and patient treatment 50 mg female viagra free shipping women's health big book of yoga amazon. The prerequisite for success in this fight is the participation of all health care professionals. Nurses and midwives, as major frontline providers of care, are in a position to contribute significantly to reducing the burden. Mastery of this material will enable nurses and midwives to respond to threats to the community, to teach their patients and members of the community effective ways of preventing infections and infectious diseases, to provide high quality and effective care to people with infectious diseases and to use appropriate measures to ensure safe practice. Each module is in two parts: theory and practice, with opportunities for self-assessment through learning activities and a workbook. The manual should be used as a package to ensure that, after training, nurses and midwives have a broad and up-to-date knowledge of infections and infectious diseases. Each section of the manual can also be used independently to develop knowledge in a specific area, and the manual as a whole can be used as a reference book in health care settings. Over the last two years, the Scottish Centre for Infection and Environmental Health has adapted the Chinese manual to make it relevant to nurses and midwives in Europe. It is intended that each module Module 1: The prevention and control of infection should consist of theory and also require practice Module 2: The Expanded Programme of for completion. An index that indicates which topics are covered • modes of transmission; and where you can find them. A glossary of terms that explains what terms • manifestations; mean; you should refer to this throughout each • complications; module. Some words or terms may be found in • risk factors / age groups affected; more than one module. Stated learning outcomes, indicating what you • methods of treatment; should achieve on satisfactory completion at the • prevention of spread; end of each module. Key words, that is, words or terms of particular • contact tracing; relevance to an individual module. The main body of the text, containing theory • rehabilitation; and factual content; the same paragraph headings • prevention strategies; and are used throughout the manual where appropriate. Learning activities, to be carried out when and infectious diseases; and indicated in the text; a workbook is provided separately for this. Revision points: these indicate that you should workbook is designed to assist you to complete stop and note some points or answer a question. The summary of key points is a reiteration of is a blank space under an activity, this should be the most important messages to absorb and used for notes. It is sources whenever possible; only the main sources recommended that in order to get the most benefit used for each module are included in the from the manual, you should not refer to this until bibliography. Further information Theory versus practical learning composition The manual is designed to be self-contained. The The manual content contains most of the theory number of other sources of information in the required to provide a firm basis of knowledge on bibliography of each module has been kept to a infections and infectious disease. The purpose of minimum; those which have been cited are the revision points is to test your knowledge on particularly useful. Try to manual is only as up-to-date as the date of respond to the revision points without referring to publication; to obtain the most up-to-date the text in the first instance, then compare your information available, visit the websites mentioned response to the information in the manual. The learning activities are intended to be more Assessment of revision points practical and are related to nursing or midwifery You can test this yourself by comparing your practice incorporating wider aspects relevant to the response to the information in the manual text. For example, you may be asked to visit a laboratory, carry out an audit in your place of work or produce a leaflet to give to patients. The learning activities are designed to further develop your knowledge and are also practical and useful. Depending on your area of practice, some learning activities will be more useful than others. Assessment of learning activities It is indicated within the text of each module when you should carry out a particular learning activity. Infection control is especially important within healthcare settings, where the risk of infection to patients is greatly increased. Good infection control techniques adopted during patient care can assist greatly in preventing or reducing avoidable History of infection control Infection control measures help hospital-acquired infections. In the 14th century, the Venetians quarantined ships arriving at their port in order to contain diseases There are important public health issues in the prevention and control such as plague. In the 19th of infection, including the general health and nutritional status of the century, Semmelweiss, a Viennese obstetrician, realized that infection public, and their living conditions, such as housing, water and sanitation was passed to patients on the hands of healthcare workers. These influence the level of infectious disease in the community, showed conclusively that infection could be greatly reduced by hand which in turn affects the level of infection of those both in and outside washing. In addition, in the 19th century separate facilities for of hospitals, thus affecting the burden on healthcare facilities. Local infection control policy manuals should be produced within Basic infection control measures individual settings in order to give guidance to staff on the are essential in everyday practice today. The introduction of antibiotics in Hospital-acquired the 1940s saw a decrease in basic measures, such as cleaning, in (nosocomial) infections everyday hospital practice, which Hospital-acquired infections, or nosocomial infections, are infections that previously had been the only defence measure for patients were not present or incubating on admission of a patient to hospital. People thought These infections can be readily diagnosed in patients who have appeared that the microorganisms that had caused many deaths had been free of signs and symptoms of infection on admission and have then gone beaten. Unfortunately it was soon discovered that these micro- on to develop infection – for example, a surgical wound exuding pus. In addition, they were These infections can cause unnecessary suffering for the patient and also able to inactivate antibiotics by developing chemicals that rendered create unnecessary costs for the health facility. Page 4 Module 1 Microbiology To begin to understand why we must undertake infection control measures we must first consider aspects of microbiology. Microbiology is broadly described as the study of bacteria, fungi, protozoa, viruses, and helminths. In studying these groups of organisms, including their are small microorganisms of simple primitive form. Bacteria many subgroups and families, we can learn how: can commonly be found living • they live within us; within our bodies and in our environment, for example in • they live in our environment; animals, soil and water. For examples of common agents so small that they are microorganisms found in healthcare settings, see Appendix 1. Knowledge of Fungi are simple plants that are parasitic on other plants and this cycle is essential in order to understand how infection can occur. A few can cause fatal All precautions and measures taken in order to prevent and control disease and illness in animals and humans. Helminths are large parasites - worms, which can be a major cause of morbidity in some countries. The cycle of infection Infectious agent Bacteria Fungi Viruses Protozoa Susceptible host Helminths Neonates Reservoir Diabetics People Immunosuppression Equipment Cardiopulmonary Water disease Elderly Portal of entry Broken skin Portal of exit Mucous membrane Excretions Gastrointestinal tract Secretions Resipratory tract Droplets Urinary tract Skin contact Means of transmission Bloodborne Airborne Droplet Common vehicle Vectorborne Portals of entry are the same as the portals of (Note: certain organisms can be transmitted through more exit and are either natural or artificial. Examples of organisms that can be spread by all of these routes are found in Appendix Means of transmission: 1). The main concerns in healthcare settings are the Reservoir: where microorganisms can be found.
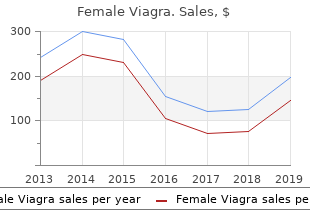
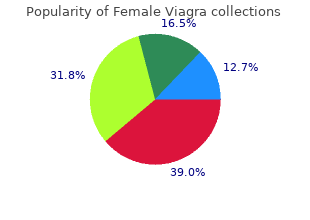
Appears agitated and distressed or when there is conflict when there is conflict B purchase female viagra 100mg without prescription menopause systems. Ignores or dismisses conflict or conflict or tension between provider tension and patient C buy 100 mg female viagra women's health center gainesville fl. Takes it upon self to solve or making conflicts or tensions explicit handle the conflict; does not make so that they can work them out the issue(s) explicit between themselves D female viagra 100 mg visa breast cancer apparel. Does not encourage the provider to appropriate instructions buy discount female viagra 100 mg menstruation jokes, making give appropriate instructions, and sure the patient is clear about next des not make sure the patient is steps and has asked any questions clear about next steps, nor asks she or he may still have whether the patient has any further questions B. Does not check with the patient on for an interpreter at any of the the need for an interpreter at any follow-up appointments of the follow-up steps C. Does not understand or does not institution’s system of service ask about the institution’s system delivery of service delivery C. Does not find out what protocols each institution/health care setting the institution requires in which work is performed B. Does not follow the documentation procedures/ guidelines of each policies/ procedures/ guidelines of institution’s interpreter office, the institution, resulting in the which may include: following possible situations: Keeping phone log Errors in follow-up activities Documenting all follow-up Mishandled priorities activities, such as follow-up Not getting paid appointments Interpreter’s office not being Completing weekly invoice of able to locate interpreter hours worked Incomplete or inaccurate Submitting documentation to the statistics at the end of the year appropriate person or filing documentation in the appropriate place and in a timely manner Keeping interpreter’s office informed of exact location (i. Does not notify patients of follow- canceled, or rescheduled up, canceled, or rescheduled appointments when requested appointments when requested B. Does not reschedule appointments patients when requested for patients when requested C. Does not observe the rules of etiquette and/or institutional norms cultural etiquette and/or (e. Ignores verbal/nonverbal cues that nonverbal cues that may indicate indicate implicit cultural content or implicit cultural content or culturally based culturally based miscommunication miscommunication (e. Does not assess the the issue, at that point in time in urgency/centrality of the issue and that particular exchange, to the becomes a barrier to goals and outcomes of the communication by: encounter: Interjecting disruptively (e. Does not assist the speaker in terms are used, assists the speaker developing explanations for in developing an explanation that ‘untranslatable’ words, instead can be understood by the listener providing explanations for the words or omitting concepts *Untranslatable words are words that represent concepts for which a referent does not exist in the society using the target language. Cannot explain the boundaries and meaning of confidentiality, and its the meaning of confidentiality, nor implications and consequences its implications and consequences B. Intentionally or unintentionally parameters of information sharing, reveals confidential information in keeping with the policies and outside the clinical parameters procedures of the institution and/or team, for example: Supervision Patient conference/continuity of care meetings Professional meetings, workshops, conferences, [taking responsibility for maintaining the anonymity of the parties by ensuring that any information shared at professional meetings does not contain identifying characteristics (e. Does not know how to deflect dealing with confidential matters inappropriate requests for that may be brought up in the information and violates community or health care setting confidentiality D. Cannot explain the concept of accuracy and completeness, and accuracy and completeness, nor their implications and consequences their implications and consequences B. Is not committed to transmitting accurately and completely the accurately and completely the content and spirit of the original content and spirit of the original message into the other language message without omitting, modifying, condensing, or adding C. Does not monitor her or his own his own interpreting performance interpreting performance D. Is unaware of and unable to personal biases and beliefs that may identify personal biases and beliefs interfere with the ability to be that may interfere with the ability impartial, and has the moral to be impartial, and does not have fortitude to withdraw if unable to the moral fortitude to withdraw if be impartial unable to be impartial B. Accepts assignments where close accepting any assignment where personal or professional ties or close personal or professional ties or strong personal beliefs may affect strong personal beliefs may affect impartiality, even when other impartiality (including conflicts of alternatives are available interest), unless an emergency renders the service necessary C. Interjects personal issues, beliefs, between provider and patient and opinions, or biases into the refrains from interjecting personal interview issues, beliefs, opinions, or biases into the interview D. Does not respect patient’s physical and maintains spatial/visual privacy privacy nor maintain spatial/visual of patient, as necessary privacy of patient B. Does not respect patient’s personal/emotional privacy: personal/emotional privacy: Refrains from asking personal Asks personal, probing probing questions outside the questions on own initiative scope of interpreting tasks Uses the role of interpreter to Does not use the role of influence a social relationship interpreter to influence a social with the patient outside the relationship with the patient interpreting encounter outside the interpreting Becomes personally involved encounter Refrains from becoming personally involved in the patient’s life** ** In small, close-knit communities, it is often not possible for an interpreter to remain personally and socially uninvolved with patients. However, interpreters should always strive to maintain the ethical and professional standards of confidentiality and impartiality while in their role. Cannot explain the meaning of professional distance, and its professional distance, and its implications and consequences implications and consequences B. Is not able to balance empathy boundaries of the interpreter role with the boundaries of the interpreter role C. Ignores patient needs or tries to needs by facilitating the use of resolve everything for the patient appropriate resources D. Becomes personally involved to involved the extent of sabotaging or compromising the provider-patient therapeutic relationship, thereby misleading the patient as to who the provider is and effectively disempowering the provider E. Creates expectations in either party either party that the interpreter role that the interpreter role cannot cannot fulfill fulfill F. Encourages and/or creates patient taking into account the social dependency on the interpreter. Initiates contact with the patient patient outside the scope of outside the scope of employment employment, avoiding personal for personal benefit benefit B. Takes on functions or provides functions or services that are not services that are not part of the part of the interpreter role interpreter role C. Is not aware of competency limits; refrains from interpreting beyond becomes involved in situations that her or his training, level of are beyond her or his level of experience, and skills, unless these training, skill, and/or experience; limitations are fully understood by and on occasions where no other the patient and provider and no source of interpreting is available, other source of interpreting is does not inform patient or available provider of these limitations D. Persists in functioning as an situations where there may be a interpreter in situations where conflict of interest there may be a conflict of interest E. Does nothing or addresses the feels strongly that either party’s situation in an ineffective, behavior is affecting access to or disruptive manner quality of service, or compromising either party’s dignity, uses effective strategies to address the situation B. Dietary flavonoids, abundant in plant-based foods, cause the population of a country is substantially have been shown to improve cognitive function. Data on per present in cocoa, green tea, red wine, and some capita yearly chocolate consumption in 22 fruits, seems to be effective in slowing down or countries was obtained from Chocosuisse even reversing the reductions in cognitive per- (www. To laureates per 10 million persons in a total of 23 my knowledge, no data on overall national cog- countries (Fig. Conceiv- exclusion of Sweden, the correlation coefficient ably, however, the total number of Nobel laure- increased to 0. Switzerland was the top per- ates per capita could serve as a surrogate end former in terms of both the number of Nobel point reflecting the proportion with superior laureates and chocolate consumption. The slope cognitive function and thereby give us some of the regression line allows us to estimate that measure of the overall cognitive function of a it would take about 0. The minimally effective chocolate dose seems to A list of countries ranked in terms of Nobel hover around 2 kg per year, and the dose–response laureates per capita was downloaded from curve reveals no apparent ceiling on the number Wikipedia (http://en. Correlation between Countries’ Annual Per Capita Chocolate Consumption and the Number of Nobel Laureates per 10 Million Population. Considering that in this instance the observed The principal finding of this study is a surpris- number exceeds the expected number by a fac- ingly powerful correlation between chocolate tor of more than 2, one cannot quite escape the intake per capita and the number of Nobel laure- notion that either the Nobel Committee in ates in various countries. Of course, a correla- Stockholm has some inherent patriotic bias tion between X and Y does not prove causation when assessing the candidates for these awards but indicates that either X influences Y, Y influ- or, perhaps, that the Swedes are particularly ences X, or X and Y are influenced by a common sensitive to chocolate, and even minuscule underlying mechanism. Obviously, ceivable that persons with superior cognitive these findings are hypothesis-generating only function (i. Given its per capita chocolate con- Prize would in itself increase chocolate intake sumption of 6. It Finally, as to a third hypothesis, it is diffi- remains to be determined whether the consump- cult to identify a plausible common denomina- tion of chocolate is the underlying mechanism tor that could possibly drive both chocolate con- for the observed association with improved cog- sumption and the number of Nobel laureates nitive function. Messerli reports regular daily chocolate consumption, status from country to country and geographic mostly but not exclusively in the form of Lindt’s dark varieties.
Do not to allow the calcium chloride solution to be sucked back into the sodium alginate pipette generic 100 mg female viagra free shipping women's health center peru il. If the calcium chloride goes into the pipette cheap female viagra 100mg with visa womens health neenah wi, it will become clogged with cross-linked ions purchase 100 mg female viagra visa menstrual bleeding for 2 weeks. Allow the students to take their creations out of the calcium chloride solution and onto a paper plate for observation purchase 50 mg female viagra breast cancer risk. Students should work together to create a poster explaining how scaffolding is the basis for tissue and organ engineering. Extension The activity may be extended by researching the types of materials used to create scaffolds and the advantages and disadvantages of each type. Students may use the resources found on selected websites, such as the Regenerative Medicine Foundation (http://www. How could the different shapes created in this activity help in organ engineering? But the media often neglects to discuss what stem cells really are, how they are being used in research and treatments, the many different kinds of stem cells and recent advances in stem cell research that may reduce or eliminate the need for controversial embryonic stem cells. Stem cells can be used as unique building blocks in bioengineering and growing tissues and organs. This activity will provide students opportunities to defne stem cells and research their characteristics. Theaching Notes This activity asks students to use the Internet to research what stem cells are and the different types of stem cells. The students will research the characteristics, advantages and disadvantages of different stem cells. To make the most effective use of student research time, suggested resources have been provided. Depending on student access to the Internet, you may choose whether to have students do this research in or out of class. After gathering and synthesizing information, the students will create a commercial to share their fndings with other students. The discussion of stem cells will culminate with a gallery walk that synthesizes the stem cell information. Sharing the rubric at the end of this lesson plan helps students meet expectations. Explain to students they will have the opportunity to defne this term and research how different types of stem cells are used in different therapies. They will use two to three resources to research this basic question and fnd out what is different between adult and embryonic stem cells. In order to move to the next section of this activity, each student will write a paragraph explaining what a stem cell is, which may be used as a formative assessment. After the students have completed their paragraph satisfactorily, students will be placed in a group of two or three students and choose to research pluripotent or multipotent stem cells. The student will be required to explain how the specifc stem cell is used and the advantages and disadvantages. Discussion: Helping Students Build Understanding and Make Connections After students share the commercials they will synthesize the information by completing a gallery walk. Place four (or more) posters on the wall with the following labels: Pluripotent Advantages, Pluripotent Disadvantages, Multipotent Advantages, Multipotent Disadvantages. Students in each group will write down as many facts on the sheet as they can remember in three minutes. After three minutes, the posters will be passed to the next group and the process repeated until all groups have written on each of the posters. Place the posters on the wall and allow students to walk around the room silently and place two checks on each paper for the strongest point. These posters will provide a visual representation of the research that can be posted in the class and referred to throughout this course. They should be shared with students in advance and may be developed with students. Theachers may adjust this rubric to ft their grading system and to emphasize different aspects of the project as appropriate for their curriculum. Extension This activity may be extended by asking students to research how stem cells may be used to combat chronic disease, such as cancer. Because this research area is evolving rapidly, online information is more likely to be up-to-date than information in print. Some options include: National Institutes of Health The National Institutes of Health has a number of resources on stem cells, including: • Current Research http://stemcells. Does not seem Shows a full Shows a good Shows partial Commercial to understand the understanding of understanding of understanding of content stem cell very the stem cell. Student uses Accuracy (of both appropriate Presents accurate Presents accurate Hard to tell if the written notes and sources. Material material 90% to material 75% to student knew the oral presentation) accurate based on 95% of the time. Student is able Student is able Student is able Student is unable to accurately to accurately to accurately to accurately Comprehension articulate the articulate most of articulate part of articulate the topic. Provides a Performs the Provides an complete Provides a simple commercial exceptional Commercial commercial that commercial that in-person for the commercial that quality falls within 30 does not meet the class and/or does meets the time seconds of the time requirements. Before delving deeper into the uses of different types of stem cells, defne the phrase “stem cell. On another sheet of paper make a chart similar to this one but with enough space to record all your fndings. Key Vocabulary • Regenerative medicine • Organ engineering • Scaffold • Bioprinting Time Required • Approximately 90 minutes to research regenerative medicine (may be done outside of class) • Approximately 60 minutes to create regenerative medicine magazine cover (may be done outside of class) • Approximately 90 minutes to present regenerative medicine covers (for class of 30 students) Materials • Computers with Internet access and print materials for research • Rubric Background Information Regenerative medicine holds the possibility of using stem cells to engineer and grow tissues and organs. In the past, if someone had a diseased bladder he or she most likely would develop kidney disease and possibly would die. But in 2001, a young boy was given a new bladder that had been grown for him in the lab. This feld of medicine continues to evolve, thus students must keep up with new advances by reading current research. Depending on student access to the Internet, you may choose to have students do this research in or out of class. After gathering and synthesizing information, the students will create a magazine cover highlighting their favorite advances in regenerative medicine. Safety Students should follow school/district Internet access guidelines to ensure safe browsing. Procedure Begin by watching a video on regenerative medicine, such as Heal, Feed, Sustain: How Biotechnology Can Help Save the World (http://www. Explain that they will be able to answer many of these questions and others after completing this project. Explain that regenerative medicine is a constantly changing feld, thus they will be using online resources to discover current advances. The student will work in groups of two to complete the following Regenerative Medicine: Changing Life handout. In order to move to the next section, the teacher may use the student sheet as a formative assessment.
Walden University 2015 Abstract Women and Thyroid Disease: Treatment Experiences and the Doctor-Patient Relationship by Laura J cheap 50mg female viagra mastercard womens health 2014 covers. Numerous factors make diagnosing and treating thyroid disease in women challenging cheap female viagra 100mg visa pregnancy 5 weeks 6 days. The standard blood test for diagnosing thyroid disease and determining treatment effectiveness is inconsistent in its accuracy cheap female viagra 50mg with amex menstrual calculator. Many women with thyroid disease are misdiagnosed or struggle with symptoms even once receiving treatment generic female viagra 100 mg free shipping women's health clinic cleveland. Although thyroid disease is highly prevalent among women and the doctor-patient relationship is known to influence treatment outcomes, there is a gap in the literature regarding the treatment experiences of women with thyroid disease and the doctor-patient relationship. The purpose of this phenomenological study was to explore female thyroid patients’ experiences of treatment and the doctor-patient relationship. Sixteen female thyroid patients, ages 18 and older and members of an international online support group, were individually interviewed via online chat. Data interpretation was guided by social constructionism and feminist theory and was accomplished via Moustakas’s analytic method. Themes related to the doctor-patient relationship were identified, including the culture of the medical profession, diagnostic bias, and gender differences in communication. Emergent themes included patient education level, patient self-advocacy behaviors, and the use of natural thyroid medication. The results of this study may contribute to positive social change by enhancing doctors’ understanding of thyroid disease in women and the influence of the doctor-patient relationship in determining positive treatment outcomes, thus equipping doctors with enriched knowledge for providing their female thyroid patients with the highest quality of care. Women and Thyroid Disease: Treatment Experiences and the Doctor-Patient Relationship by Laura J. Ruth Crocker—Thank you so much for sharing your wisdom with me during this long journey. We will overcome the debilitating effects of thyroid disease and help to ensure better outcomes for individuals yet to be diagnosed. Across cultures, the prevalence of thyroid disease is much higher among women than among men (Canaris, Manowitz, Mayor, & Ridgway, 2000; Cassidy, Ahearn, & Carroll, 2002). In fact, women have an estimated 1 in 7 chance of developing thyroid disease (Godfrey, 2007). A number of factors make proper diagnosis and treatment of thyroid disease challenging. In addition, as thyroid dysfunction produces symptoms similar to those of other disorders (e. In the face of such challenges, a doctor-patient relationship based on mutual trust and collaboration helps to ensure positive treatment outcomes (Houle, Harwood, Watkins, & Baum, 2007; Munch, 2004). In addition, effective communication between doctors and patients is critical in both the diagnosis and management of thyroid disease (Shimabukuro, 2008; Simmons, 2010). However, the culture of the medical profession, diagnostic bias, and gender differences in communication may interfere with doctor-patient discourse (Cheney & Ashcraft, 2007; Hamberg, Risberg, & Johansson, 2004; Hoffmann & Tarzian, 2001; Kaiser, 2002; Munch, 2004). An exploration of women’s experiences in the treatment of thyroid disease, especially relative to these three points, may contribute to better understanding on the part of doctors and thus more effective doctor-patient communication and relationships. Despite the pervasiveness of thyroid disease in women and the importance of the doctor-patient relationship in positive treatment outcomes, there is a gap in the literature regarding the treatment experiences of women diagnosed with thyroid disease, particularly regarding the doctor-patient relationship. Therefore, the purpose of this phenomenological study was to explore female thyroid patients’ experiences of treatment and the doctor-patient relationship. The phenomenological research approach was used, as it is designed to examine the meaning of experiences about a particular phenomenon (e. The theoretical perspectives used to guide data interpretation included feminism and social 3 constructivism. More specifically, the following issues were addressed in regard to their relationship with women’s treatment experiences: (a) the culture of the medical profession (see Kaiser, 2002; Thomas, 2001), (b) diagnostic bias (see Hamberg et al. The following paragraphs provide a review of the literature relevant to the study, followed by the problem statement, the purpose and nature of the study, research questions, conceptual framework, definition of terms, assumptions and limitations, and the significance of the study. Background of the Study The incidence of thyroid disease is higher than previously thought (Canaris et al. Across cultures, the prevalence of thyroid disease is much higher in women than men (Canaris et al. Approximately 1 out of every 7 women develops thyroid disease, and its prevalence increases with age (about 20% in women over age 60; Godfrey, 2007). The two predominant conditions resulting from thyroid disease are hyperthyroidism and hypothyroidism, with Grave’s disease and Hashimoto’s disease, respectively, as the most common causes (Zeitlin et al. In the United States, the most common cause of hyperthyroidism is Grave’s disease, an autoimmune form of thyroid disease (Bunevicius & Prange, 2006). Individuals with hyperthyroidism experience heat intolerance, hot flashes, absent menses, insomnia, decreased libido (Godfrey, 2007), rapid heartbeat, sweating, and tremors (Aslan et al. In the United States, the most common cause of hypothyroidism is Hashimoto’s disease, an autoimmune form of thyroid disease (Erdal et al. Individuals with hypothyroidism experience fatigue (Bono, Fancellu, Blandini, Santoro, & Mauri, 2004), lethargy, apathy, difficulty concentrating (Aslan et al. In extreme cases, the individual may experience slowing of thought processes, progressive cognitive impairment, hallucinations, and delusions (Bono et al. Furthermore, abnormalities in thyroid function present with symptoms similar to those of other disorders and can be mistaken for other conditions (Canaris et al. For example, hyperthyroidism and hypothyroidism are frequently misdiagnosed as anxiety and depressive disorders, respectively (Aslan et al. Postpartum thyroiditis, which affects more than 8% of women, is sometimes mistaken for depression (Fassier et al. In older patients, symptoms of hyperthyroidism and hypothyroidism often lead to inaccurate diagnoses of menopause or dementia (Godfrey, 2007; Shimabukuro, 2008). Thus, it is vital that physicians conduct a thorough assessment of their patients, including an ongoing discussion of symptoms, to ensure proper diagnosis and treatment. Although antithyroid drugs have been used for over 60 years, remission rates are variable, and relapses are frequent. However, some experts recommend the addition of T3 (liothyronine; name brand Cytomel) due to its antidepressant effects (Dayan, 2001; Joffe, 2006). As previously mentioned, proper treatment of thyroid disease is dependent upon accurate diagnosis. Misdiagnosis of thyroid disease delays treatment and can result in progressive psychological and physiological problems (Heinrich & Grahm, 2003; McDermott & Ridgway, 2001) including psychosis (Gaitonde, Rowley, & Sweeney, 2012; Heinrich & Grahm, 2003) and potential heart failure (Hak et al. These risks highlight the importance of an effective doctor-patient relationship in ensuring proper diagnosis and positive treatment outcomes. The treatment experiences of women with thyroid disease might be best examined from social constructionist and feminist viewpoints, as both worldviews emphasize individuals’ experiences in social contexts (Docherty & McColl, 2003; Fernandes, Papaikonomou, & Nieuwoudt, 2006; Hearn, 2009). From a social constructionist viewpoint, patients’ interpretations of their illness experience are important in understanding and treating illness. The feminist viewpoint suggests that female patients’ interpretations of their experiences are influenced by social constructs (e. Because social constructs come from patients, physicians, and social institutions (Hearn, 2009), women’s experiences with thyroid disease diagnosis and management may be influenced by the culture of the medical profession, diagnostic bias, and gender differences in communication. Culture of the Medical Profession In the Western medical profession, health-care practitioners are taught via the medical model to base their diagnostic and treatment decisions on “objective evidence” of disease (e.
These estimates day discount female viagra 50 mg line women's health clinic calgary, and the optimism and energy we pour into doctor-diagnosed arthritis order female viagra 50mg with amex workout tips women's health. Prevalence estimates for systemic lupus 2 problems and heart trouble are among the top erythematosus range as high as 1 discount 50mg female viagra fast delivery womens health visit. In addition female viagra 100mg with amex menopause sweating, complica- trouble walking a distance equal to walking from 294,000 tions from treatment of arthritis can result in death. Another instance of scientifc discov- a request for letters of interest open to every- Trelated diseases. Scientifc research ery is the knowledge made available by genomics, one everywhere to submit their scientifc ideas We are collaborating and development holds the key to fnding better proteomics, imaging and other technologies. Please building For almost 70 years, the Arthritis Foundation has knowledge to accelerate real-world applications of refer to the appendices for more information about initiated and supported scientifc discoveries that scientifc fndings to improve human health. The Arthritis Foundation continues to with information to choose the correct biological scientifc strategy includes three interconnected lead the way in advancing scientifc discoveries and targets so that a therapeutic product will work scientifc pillars: delivering on discovery, decision seeking solutions that will positively impact the lives against the disease it is intended to treat. Our commitment to fnding a For this strategy, arthritis refers to more than 100 For our scientifc strategic planning process, cure is unwavering. Together, we can have “arthritis on the For the purposes of this scientifc strategy, scien- of interviews with a wide range of experts and run” by accelerating the movement of scientifc tifc discovery includes a continuum of scientifc constituents, including people with arthritis and 13 knowledge to a faster cure. Each stage related diseases, fndings documented in scientifc research of scientifc research and development can infu- ence the other stages. Each scientifc discovery for arthritis and stage is informed by people with arthritis and Scientifc Strategy Goals related diseases. People with arthritis beneft from The scientifc strategy is the direction the Arthritis Foundation Science Department is going each stage in the continuum. The goal for each pillar is the impact of the inputs and outputs for each pillar (see Figures 2-4). To illustrate the continuum of scientifc discovery, consider the following examples. Decision Studies Scientific Making Discovery Continuum Population Systematic Health Reviews/ Surveillance Synthesis & Studies 10 “Science has Arthritis on the Run. In the past, it took an average complexities of clinical research and practice, as Tof 17 years for only 14 percent of new well as the many other challenges that occur on the scientifc discoveries to be available to the people in scientifc discovery continuum. A key to medicines and therapies for the prevention, early delivering on discovery is that each team — no matter detection, diagnosis and treatment of disease. Whether we main repository of medical images, patient data are facilitating better evidence-based decision and bio-samples. Data from the Million candidates to: development of new diagnostics and pharmaceutical Veteran Program26 are being analyzed to create a. Plan for translation of scientifc knowledge into the products people need to treatments. Measure metrics that matter and validating the most promising biological targets diagnosing arthritis earlier. When the algorithms are Provide leadership and oversight in building collaborative, interdisciplinary teams who 03 for rheumatoid arthritis and systemic lupus erythe- confrmed, clinicians can use the decision-making achieve meaningful results and accelerate scientifc discovery to fnd a faster cure for matosus (lupus). These new targets will inform the tools to diagnose people with arthritis and identi- people with arthritis and related diseases development of new diagnostics and drugs to treat fy those who need to be referred to rheumatol- Engage people with arthritis and related diseases in the scientifc discovery process 04 people with rheumatoid arthritis and lupus. Eventually the tools will be ready to use for telehealth and may even lead to pre-clinical diagno- In our collaborations with the Patient-Centered sis. The data and Discovery and translation of scalable new products, tools and technologies of the process, from study design to study imple- methods for this demonstration project are made for diagnostics, interventions and a cure mentation and interpretation of the fndings. Every possible by years of scientifc discovery and technol- person, no matter how arthritis affects their life, is ogy research and development. The demonstration Improved decision making and better lives through improved prevention, welcome to participate. There is an ongoing need for updated and awareness and use of advanced medical imaging. The Bone and Joint Initiative published a a combination of metrics, but not enough data are burden of disease report that included economic available to fully answer the questions. Although many of treating these individuals in addition to the cost to physical and social benefts are enjoyed by people society in the form of decreased wages is estimated playing sports, more than 2. If the arthritis Health to fnd ways to answer questions that have outcomes associated with chronic conditions registries in the United States agree to collecting not yet been answered, as well as continuing to such as arthritis and related conditions standardized core metrics, then the data can be update existing facts as new information becomes A specifc source of data to produce metrics for public pooled together to have statistical power to answer available. The Arthritis Foundation is a Healthy health surveillance and health research is registries. Registries provide People Consortium Partner to take actions to A registry is a collection of information about individ- overall acceleration of the research process and also strengthen policies and improve practices that are ual people, usually focused around a specifc diagno- 15 expertise from existing efforts such as Outcome provide data to design more effective clinical trials. For highly reliable, precise measures of patient-reported injury and premature death. One option discretionary social activities and satisfaction with prevention and treatment of comorbidities, such as arthritis can be prevented. Each registry has a focus for developing such a pain index is by combining social roles. Travel to in-person trainings will be research for arthritis and related diseases covered for both trainees and experts. This training has a strong interdisciplinary pipeline program would be symbiotic with existing training Tof scientists to implement our frst two and mentoring programs. For example, this new program can opportunities is a challenge for many investigators. This challenge was intended to crowd- and development for arthritis and related diseases source human genetics with the ultimate objective by recruiting 1) trainees who are experts in arthritis of identifying genetic predictors that could improve research but would beneft from training in interdis- treatment for those suffering from rheumatoid ciplinary scientifc research and development skills, arthritis. To steer the tors interested in applying their talents to arthritis investigators into the validation phase, Sage Bionet- research, and would beneft from understanding works quickly realized the need to provide training the history and current needs in the feld of arthri- about the history and needs of rheumatoid arthritis tis research (Figure 4). The Arthritis Foundation will research so that investigators new to arthritis could provide curriculum for the interdisciplinary trainings build upon existing knowledge and improve the and identify experts who will be paid for their time deliverables being produced. Arthritis research history and current needs Trainees and experts Curriculum b. Interdisciplinary skills to turn scientifc discoveries into real-world uses 03 Pilot test the training program Local connections are strengthened 04 Evaluate the pilot training program Quality proposals Successful scientifc research and development that accomplishes a 05 Revise the training program based on evaluations specifc scientifc goal 06 Implement the training program including ongoing evaluation 07 Track the impact of the training program Scientifc research pipeline is strengthened and scientifc discovery is catalyzed and accelerated for arthritis and related diseases Building Human Capital: How You Can Be Involved 01 Spread the word about the interdisciplinary training program 02 Be a trainee 03 Identify and provide lessons learned from other mentoring and training programs 04 Volunteer to be an expert who develops or teaches the curriculum 05 Volunteer to assist with planning, implementation and/or evaluation of the program 06 Donate and/or raise funds to support the mission of the Arthritis Foundation 24 “Science has Arthritis on the Run” Arthritis Foundation Scientifc Strategy 2015-2020 25 Goals and Targets he Arthritis Foundation’s mission is to improve lives through leadership in the prevention, control and cure of arthritis and related diseases. The scientifc strategy is the direction the Arthritis Foundation Science Department is going during 2015-2020 to bring everyday wins now and in the future for Ta lifetime of better. Each pillar is designed to champion and accelerate progress for achieving our mission. The goal for each pillar is the impact of the inputs and outputs for each pillar (see Figures 2-4). The three pillars and their goals are as follows: Pillar #1: Delivering on Discovery Improved decision making and better lives through improved prevention, earlier diagnosis and new treatments to prevent, control and cure arthritis and related diseases Pillar #2: Decision Making With Metrics Fact-based metrics for decision making and guiding actions to improve the health of people across the lifespan with arthritis and related diseases Pillar #3: Building Human Capital Scientifc research pipeline is strengthened and scientifc discovery is catalyzed and accelerated for arthritis and related diseases In collaboration with other organizations, the Arthritis Foundation Scientifc Strategy 2015-2020 is contribut- ing to the achievement of the following Healthy People 2020 targets. One of the criteria for selecting these targets is that existing data sources are available to measure progress on meeting the targets.
Purchase female viagra 50 mg fast delivery. పక్కన చిన్నపిల్లలు లేకుండా మగవారు మాత్రమే ఈ వీడియో చూడండి ¦ Mana Telugu.