
Wichita State University. H. Jorn, MD: "Buy Rabeprazole - Best Rabeprazole no RX".
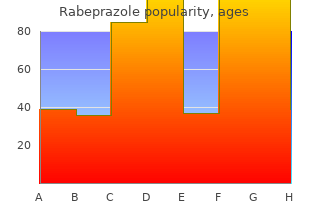
Accordingly buy rabeprazole 10mg with amex gastritis fiber diet, the rate of systemic absorption is greatest with intercostal nerve blocks buy generic rabeprazole 10mg on-line gastritis icd 9, followed in decreasing order by caudal and epidural injections cheap rabeprazole 10mg on line stomach ulcer gastritis symptoms, brachial plexus block order rabeprazole 10 mg without prescription gastritis diet how long, and femoral and sciatic nerve blocks (Table 22-6). Thus, the same amount of local anesthetics injected would result in unequal peak plasma levels depending on the site of drug delivery. For a given site of injection, the rate of systemic absorption and the peak plasma level are directly proportional to the dose of local anesthetic deposited. In general, more potent lipid-soluble agents are associated with a slower rate of absorption than less lipid-soluble compounds (Fig. Local anesthetics exert direct effects on vascular smooth muscles in a concentration-dependent manner. At low concentrations, more potent agents appear to cause more vasoconstriction than less potent agents, thereby decreasing the rate of vascular absorption. At high concentrations, vasodilatory effects seem to38 predominate for most local anesthetics. The pattern of distribution is largely dependent on organ perfusion, the partition coefficient between compartments, and plasma protein binding. Organs that are well perfused,82 such as the heart and the brain, have higher drug concentrations. Unfortunately, they are also the organs most seriously affected by local anesthetic toxicity. Aminoesters are hydrolyzed by plasma cholinesterases and aminoamides are transformed by hepatic carboxylesterases and cytochrome P450 enzymes. Severe liver disease may slow the clearance of aminoamide local anesthetics and significant drug levels may therefore accumulate. Bupivacaine is a more lipid-soluble and more potent agent with less systemic absorption over time. Nonetheless, pharmacokinetics are difficult to predict in any given circumstance because both physical and pathophysiologic characteristics will affect the individual pharmacokinetics. There is some evidence for increased systemic plasma levels of local anesthetics in the very young and in the elderly owing to decreased clearance and increased absorption ; however, the correlation of systemic blood levels between the84 dose of local anesthetic and weight is often inconsistent (Fig. Effects85 of gender on clinical pharmacokinetics of local anesthetics have not been well defined, although pregnancy may decrease clearance. Pathophysiologic86 87 states such as cardiac and hepatic disease will alter expected pharmacokinetic parameters (Table 22-10), and lower doses of local anesthetics should be used for these patients. As expected, renal disease has little effect on pharmacokinetic parameters of local anesthetics (Table 22-10). All of these factors should be considered when using local anesthetics and minimizing systemic toxicity, the commonly accepted maximal dosages (Table 22-9) notwithstanding. Arterial and pulmonary concentrations of the enantiomers of bupivacaine after epidural injection in elderly patients. They all take advantage of their ability to attenuate or block pain and other noxious stimuli. When applied topically to the skin, a eutectic mixture of lidocaine and prilocaine reduces the sharp, painful sensation associated with needle insertion and intravenous catheter placement, particularly in the pediatric population. In the awake patient, aerosolized benzocaine and viscous lidocaine directed at the mucosal surface can help blunt the protective reflex responses associated with airway instrumentation (see Chapter 28). In addition, lidocaine can be given intravenously to decrease the incidence and the severity of pain associated with propofol administration (see Chapters 19, 31). Likewise, intravenous lidocaine may also help to reduce the hemodynamic response to tracheal intubation and extubation. For a wider and greater area of coverage, a regional anatomic approach to anesthesia and analgesia can be used. This can be accomplished either by intravenous administration of local anesthetics to a limb under pneumatic compression (Bier block) or by direct application of local anesthetics to individual peripheral nerves (nerve blocks). Local anesthetics can be deposited centrally near the nerve roots, either intrathecally in the lumbar cistern or epidurally in the thoracic, lumbar, and caudal regions of the spine (see Chapter 35). Alternatively, injections can be made peripherally at the plexus, such as at the brachial or lumbar plexus block or on the nerve fibers (see Chapter 36). The duration of the anesthesia and analgesia is dependent on the type of local anesthetics 1456 used, though it can be extended with continuous infusion through an indwelling catheter. Surveys from France and the United States of over 280,000 cases involving regional anesthesia show an incidence of seizures of approximately 1/10,000 with epidural injections and 1457 7/10,000 with peripheral nerve blocks. Nonetheless, in an analysis of closed malpractice claims in the United States from 1980 to 1999, epidural anesthesia (primarily obstetrical) constituted all of the cases of death or brain damage resulting from unintentional intravenous injection of local anesthetic. However, although all local anesthetics can cause hypotension, dysrhythmias, and myocardial depression, more potent agents (bupivacaine, ropivacaine, and levobupivacaine) are predisposed to devastating outcomes, such as fatal cardiovascular collapse and complete heart block (Fig. In animal models, both ropivacaine and levobupivacaine appear to exhibit 30% to 40% less cardiovascular toxicity than bupivacaine on a milligram-to-milligram basis (Fig. Although local anesthetics can directly cause major disturbances to the heart, their effects on other components of cardiovascular systems may be just as important. Disruption to the arterial baroreflex in the brainstem by bupivacaine can lead to attenuation of the heart rhythm response to changes in blood pressure. In the periphery, vasoconstriction occurs at subclinical doses and vasodilation at higher doses. Figure 22-12 Success of resuscitation of dogs after cardiovascular collapse from intravenous infusions of lidocaine, bupivacaine, levobupivacaine (L-bupiv), and ropivacaine. Success rates were greater for lidocaine (100%) compared to ropivacaine (90%), levobupivacaine (70%), and bupivacaine (50%). Required doses to induce cardiovascular collapse were greater for lidocaine (127 mg/kg) compared to ropivacaine (42 mg/kg), levobupivacaine (27 mg/kg), and bupivacaine (22 mg/kg). Cardiac resuscitation after incremental overdosage with lidocaine, bupivacaine, levobupivacaine, and ropivacaine in anesthetized dogs. Both levobupivacaine and ropivacaine required significantly greater serum concentrations than bupivacaine. Systemic toxicity of levobupivacaine, bupivacaine, and ropivacaine during continuous intravenous infusion to nonpregnant and pregnant ewes. The central nervous system and cardiovascular effects of levobupivacaine and ropivacaine in healthy volunteers. First, bupivacaine has an inherently greater affinity for binding resting and inactivated sodium channels than lidocaine. This slow rate of dissociation prevents a complete recovery of the channels at the end of each cardiac cycle (at the physiologic heart rate of 60 to 80 beats/min), thereby leading to an accumulation and worsening of the conduction defect. In contrast, lidocaine fully dissociates from sodium channels during diastole and little accumulation of conduction delay occurs (Fig. It is widely accepted that local anesthetics bind and disrupt the normal function of the heart-specific voltage- gated sodium channel, Na 1. Local anesthetics have been shown to antagonize the currents of other cations, primarily calcium and potassium.
The physiology of steep Trendelenburg positioning is well tolerated by healthy patients rabeprazole 10 mg overnight delivery gastritis symptoms diet,196 but this cannot be assumed for those with serious comorbidities generic rabeprazole 20mg with mastercard gastritis diet virut. Although no formal guidelines exist generic 10 mg rabeprazole with amex gastritis diet ���, additional monitoring for patients with cardiac disease (e discount 20 mg rabeprazole otc gastritis diet ������. Respiratory effects of robotic prostatectomy are numerous and often require considerable adjustments to mechanical ventilation parameters. Endotracheal tube cuff location should be just beyond the vocal cords to minimize the potential for developing a main stem intubation with the cephalad shift of the diaphragm and mediastinum from the combination of head-down positioning and pneumoperitoneum. One study reported an average 8% lower tidal volumes, 22% higher respiratory rates, and 38% higher peak inspiratory pressures to maintain similar end-tidal carbon dioxide levels, but lower oxygen saturation during robotic compared to open retropubic radical prostatectomy. Potential adverse effects on intraocular pressure of head-down positioning in at-risk patients (e. Despite all these physiologic perturbations, the need to convert from laparoscopic/robotic assisted to open techniques for major urologic procedures is remarkably infrequent. This 3569 is often made more complicated by urine from the bladder neck’s spilling directly into the operative field, obscuring the surgeon’s view and impeding progress. Anticipation of this problem by the anesthesiologist can assist the surgeon through cautious fluid restriction, particularly prior to urethral anastomosis. A generally restrictive approach to fluid administration may also attenuate the development of mild facial, periorbital, and even occasionally laryngeal edema associated with prolonged steep lithotomy position. Transurethral Surveillance and Resection Procedures Transurethral endoscopy is a commonly used, relatively noninvasive surgical tool in the armamentarium of the urologist that can play an important role in the management and treatment of urothelial cancers (e. Nonetheless, about 50% of patients with a resected bladder cancer will develop another bladder or ureteral cancer in the future. Cardiovascular and pulmonary status should be carefully assessed to evaluate the patient’s ability to tolerate the intravascular volume changes associated with the procedure. Patients on anticoagulant therapy may not be candidates for spinal anesthesia, depending on the indication for anticoagulation. The risk of stopping the anticoagulant perioperatively may or may not be worth the advantages of spinal anesthesia for a particular patient. Combined spinal–epidural techniques or general anesthesia may have advantages if the length of surgery is unpredictable. Notably, the lower central venous pressure associated with regional anesthesia may actually increase the likelihood of significant irrigation fluid absorption. Body temperature 3571 decreases approximately 1°C per hour of surgery, and shivering occurs in 16% of patients who receive room-temperature irrigation fluids. Hypothermia does not develop if irrigation solutions are warmed to body temperature. Average blood loss is 2 to 4 mL/min,206 but individual bleeding rates can be difficult to assess owing to mixing with irrigating fluid. The patient’s vital signs may be useful to guide transfusion,207 but, with prolonged resections, serial assessments of hemoglobin level are advisable. Awake patients with a neuraxial anesthetic may complain during surgery of new- onset pain localized to the lower abdomen and back. Thromboplastin, a thrombogenic stimulant found in high concentrations in prostate cancer cells, can rarely trigger disseminated intravascular coagulation. Treatment of these conditions is supportive and may include transfusion of coagulation factors and platelets. Cystoscopy and ureteroscopy are rarely associated with significant complications, and perioperative considerations should generally parallel those for the disease being screened for or managed (see related sections). Transurethral Bladder Tumor Resection During any simple cystoscopy or ureteroscopy procedure, abnormal tissue may require one or more planned or unanticipated diagnostic biopsies or biopsy/resections. For this reason, muscle relaxation is preferred during general anesthesia, particularly in lateral wall resections, where the obturator nerve may be stimulated by electrocautery, producing a violent contraction of the ipsilateral thigh muscles. Neuraxial anesthesia to the T9 to T10 dermatomal level also provides adequate anesthesia for the procedure and prevents the obturator reflex. Postoperative pain is usually minimal and responds well to nonopiate and opiate medications. Laser techniques have advantages over traditional electrocautery approaches, particularly related to traditional irrigation fluid restrictions. Furthermore, the potential for systemic absorption may be reduced owing to the lower irrigation infusion rates and pressures necessary for laser procedures. Irrigating Solutions and Transurethral Resection Syndrome Key to a surgeon’s endoscopic view during transurethral procedures is a visually clear irrigating solution, infused with a pump or via gravity (and drained away) to flush out blood and resected tissue and keep space between structures. The crystalloids have current- dispersing properties owing to their ionic characteristics that make them unsuitable for use with unipolar electrocautery. When absorbed in significant amounts, nonelectrolytic irrigation solutions combine electrolyte disturbances with hypervolemia. Notably, newer transurethral bipolar electrocautery and laser techniques now allow irrigation with isotonic crystalloid solutions (e. Of available irrigating solutions, distilled water is rarely utilized owing to its hypotonicity. Water intoxication with distilled water rapidly causes severe hyponatremia leading to hemolysis, hemoglobinemia, and renal failure. Glycine, an amino acid normally metabolized to ammonia, may cause a depressed mental status and even coma (due to hyperammonemia) that can last 24 to 48 hours postoperatively. In the awake patient with a regional block, a classic triad of symptoms has been described that consists of an increase in both systolic and diastolic pressures associated with an increase in pulse pressure, bradycardia, and mental status changes. First, the surgeon should be informed of the patient’s status change so that the procedure can be completed or terminated as quickly as possible. Symptomatic patients with serum sodium concentrations less than 120 mEq/L should have their extracellular tonicity corrected with hypertonic saline. Sodium chloride in a 3% solution should be infused at a rate no greater than 100 mL/hr. Serum electrolytes should be followed closely and the hypertonic saline discontinued when the patient is asymptomatic or serum sodium concentration exceeds 120 mEq/L. Treatment with hypertonic saline has been associated with development of demyelinating central nervous system lesions (central pontine myelinolysis) owing to rapid increases in plasma osmolality, and this approach should be reserved for patients with severe, life-threatening symptoms. Up to 50% of patients with an initial stone episode will have a recurrence within 5 years. Stones form when the concentration of stone-forming salts in the urine is elevated (e. This results in supersaturation of the urine with salts, allowing crystals to form and grow, particularly in situations where urine volume is low. This pathophysiology explains the principles of the medical management of kidney stones: increasing urine volume and maneuvers to restore urinary salt balance through dietary and medical treatment. Ultrasound imaging is also informative for stones in the kidney and proximal ureter but cannot show the distal ureter and may miss smaller stones.
China Clay (Kaolin). Rabeprazole.
- Diarrhea, ulcers and inflammation in the colon (chronic ulcerative colitis), and other conditions.
- What is Kaolin?
- How does Kaolin work?
- Dosing considerations for Kaolin.
- Soreness and swelling inside the mouth, caused by radiation treatments.
- Are there any interactions with medications?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96093
Occipital region bones have the maximum thickness rabeprazole 10 mg fast delivery gastritis diet oatmeal cookies, and the temporal bones have the minimum thickness generic rabeprazole 10 mg otc gastritis diet book. It’s the lamina externa or the external plate buy cheap rabeprazole 20 mg chronic gastritis recovery time, substantia diploica or the spongeous matter which has a lot of vessels – especially vv 20 mg rabeprazole visa gastritis weed. As it goes deeper, this tunica forms the falx cerebri or the crescent of the brain and with its help it divides cerebral hemispheres from each other; falx cerebelli or the crescent of the cerebellum divides the cerebellar hemispheres, and tentonum cerebelli or the tent of the cerebellum separates the occipital lobes of the cerebral hemispheres from the cerebellum. These processes of dura mater form channels for the drainage of venous blood from the cranial cavity which are called venous sinuses. Arachnoidea encephali or the arachnoid membrane contains blood vessels and continues from one gyrus to another without going in. Spatium subarachnoidaie or subarachnoid space stores cerebrospinal fluid in its subarachnoid cisterns or cisternae subarachnoidaie. Has the most amount of cerebrospinal liquid between all the listened above spaces. Lymph drainage of this area is performed through nodi auriculares anteriores, which are located a little a bit more forward than the tragus of the ear. Lymphatic vessels traverse into the fossa pterygopalatina and fall into a deeper facial lymph nodes, or nodi faciales profundi. Below it you can find a similar space - the infratemporal fossa or fossa infratemporalis, which communicates with the frontal fossa pterygoidea. Interfascial temporal space, spatium temporale inteifasciale, is located between the superficial and deeper temporal fascia plates; it also contains adipose tissue. Cellular tissue also can be found between superficial and deep temporal fasciae and the temporalis muscle. Musculoskeletal temporal space is located between the inner surface of the temporal muscle and periosteum. The structure of the bones of the skull and mastoid process in adults and children. The smallest thickness is located in the temporal region within the squamous part of the temporal bone (pars squamosa ossi temporalis), while the thickest area is found in the occipital region. The bones of the skull have a major difference when compared with the rest of the bones of the skeleton: they do not regenerate. Bones of the skull have three layers: 1) The outer plate (lamina externa) consists of a compact matter about 1 mm thick. On the inner side of the skull you can find sulci arteriosi, which provide the possibility of close contact of dura mater’s vessels with the inner plate. Inside the mastoid area you can run across the smooth triangular shape, which is called the Shipo’s triangle. The boundaries of the triangle Shipo are defined by the next boundary: top limit is the continuation of the upper edge of the zygomatic arch, rear limit is the frontal edge of the mastoid tuberosity (tuberositas mastoidea), front limit is suprameatic spine and drum-mastoid fissura (spina suprameatum et fissura tympano-mastoidea). Neonatal cranial bones are thin, easy to bend, and are connected together with fibrous membranes. As a result, the head can change its shape when pressure is applied which is critical when the child moves though birth passway. Olfactory threads (filae olfactoriae which belong to the first pair of cranial nerves) go through its holes; 2. It links with the nasal cavity with venous anastomoses between the nasal cavity and the superior sagittal sinus. Impressiones digitae are the result of brain gyruses and cranium developing in close contact. Inside the middle cranial fossa, which is anteriorly limited with the smaller wings of the sphenoid bone, posteriorly – with the pyramid of the temporal bone and partially also with the Turkish saddle, you can locate: 1. Posterior fossa is limited by the pyramid of the temporal bone, slope and cruciform elevation, eminentia cruciata. The following formations are defined on the external cranium base: 1) foramen magnum, 2) foramen condyloideum: it serves as a connection between sinus sigmoideus and plexus venosus of the neck area; 3) canaiis hypoglossi with the same-called nerve 4) foramen mastoideum, 5) foramen stylomastoideum, stylomastoid hole: n. The Brain The cerebral hemispheres: the large brain is divided into two hemispheres: the right (hemispherium dextrum) and the left (hemispherium sinistrum). Cerebral hemispheres have superolateral surface (facies superolateralis), the bottom surface (facies inferior) and the medial surface of the brain (facies medialis). Each hemisphere is divided into pallium or cortex, the olfactory brain (rhinencephalon) and basal (subcortical) nucleui lying deep in the medulla hemisphere. Hemispheres are separated by the longitudinal fissure of the brain (fissura longitudinalis cerebri). Lobes: Each pallium is divided into four lobes: the frontal lobe (lobus frontalis), upper lobe – parietal lobe (lobus parietalis), rear lobe – occipital lobe (lobus occipitalis), lateral lobe – temporal lobe (lobus temporalis). Front has the frontal pole (polus frontalis), rear - with the central sulcus (sulcus centralis), lower part - the lateral sulcus (sulcus lateralis). Front has the central sulcus (sulcus centralis), lower part - the lateral sulcus (sulcus lateralis), rear – an imaginary line drawn between sulcus parietooccipitalis and incisura preoccipitalis. The front has temporal pole (polus temporalis), upper part - the lateral sulcus (sulcus lateralis), rear - an imaginary line drawn between sulcus parietooccipitalis and incisura preoccipitalis. Front has an imaginary line drawn between sulcus parietooccipitalis and incisura preoccipital, bottom and rear - occipital pole (polus occipitalis). Sulci: Central (Rolando’s) sulcus - sulcus centralis, which separates the frontal lobe and the parietal. The lateral sulcus - sulcus cerebri lateralis - separates the temporal lobe and the parietal. The frontal lobe has two longitudinal sulci – upper sulcus, sulcus frontalis superior, and lower sulcus, sulcus frontalis inferior. Sulcus interparietalis separates the inferior parietal lobule from the superior one. There is a sulcus in the front of the occipital lobe – it’s sulcus parietooccipitalis. Temporal lobe has 3 sulci: the upper one, middle one and lower one -sulci temporales superior, medius et inferior. It’s divided into an intermediate brain, midbrain, pons and medulla oblongata (Fig. Intermediate brain: it has visual hillocks - thalami optici, pars mamillaris hipothalami, epithalamus, metathalamus. The midbrain (mesencephalon) has the next formations: corpora quadrigemina, pedunculi cerebri, isthmus of rhomboid brain - isthmus rombencephali. In the front pons is limited with pendiculi cerebri, in the rear with the medulla oblongata. Medulla oblongata: it has an anterior medium fissure in the front and the posterior transversal fussier in the rear. On the outside the pyramid is limited with the front side sulcus, olive itself lies in the direction to the surface. On the rear surface of the medulla oblongata, by the sides of the medium fissure you can find two sulci: posterior lateral sulcus and posterior intermediate sulcus. Beginning from there, about 18-20 olfactory filaments penetrate through the ethmoid plate into the anterior cranial fossa, where the nerve enters into the olfactory bulb and then proceeds by the olfactory tract.