
University of Minnesota-Crookston. G. Grubuz, MD: "Purchase Triamterene - Proven Triamterene".
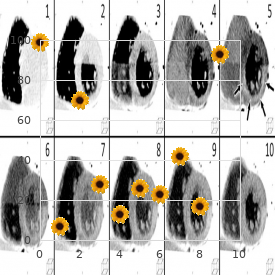
Overpenetrated film (especially portable radio- technique graphs and films on patients with very thin body habitus) order triamterene 75 mg with visa arrhythmia 101. There is striking pneumothorax (straight arrows) resulting the lungs associated with coarse intersti- hyperlucency of both lungs generic 75mg triamterene fast delivery heart attack quizlet. High frequency of abscess and cavity formation (rare in pneumo- coccal pneumonia) order triamterene 75 mg visa blood pressure 7550. Pneumococcal pneumonia Appearance similar to Klebsiella pneumonia although cavitation is rare cheap triamterene 75 mg with mastercard blood pressure 120 0. Haemophilus influenzae Most often develops in compromised hosts (chro- pneumonia nic pulmonary disease, immune deficiency, alcoho- (Fig C 17-2) lism, diabetes). Lung abscess Lobar expansion in an acute lung abscess (large (Fig C 17-3) mass, usually with cavitation) is probably related to air trapping by a check-valve mechanism in the communicating airway. Bronchogenic carcinoma Any large space-occupying mass that occupies a (Fig C 17-4) significant volume or is contiguous with a fissure. Downward bulging of the minor idation with downward bulging of the minor fissure (arrow) due to enlargement of the right upper lobe. Appearance of massive lobar enlarge- mottled opacity over the right upper lung represents ment in a 30-year-old asymptomatic man. The patchy air densities in the empyema indicate commu- nication with the bronchial tree. Charac- teristic Golden’s S sign in right upper lobe collapse (upper laterally concave segment of the S is formed by the elevated minor fissure; lower medial convexity is caused by the tumor mass responsible for the collapse). An opaque foreign In adults, collapse is usually associated with body may be detectable. Bizarre variety of causes in children (who more commonly present with overaeration of the lung distal to the site of obstruction due to collateral air drift). Typical reverse S-shaped curve (Golden’s sign) representing collapse of the right upper lobe associated with malignant bronchial obstruction. Advancing the tube too far (into the bronchus endotracheal tube intermedius) occludes the left main-stem bronchus. Frequent complication of abdominal and thoracic surgery, anesthesia and respiratory depressant drugs, and infectious diseases (eg, tetanus) that produce respiratory depression and impaired clearance of tracheobronchial secretions. Inordinately low posi- tion of the endotracheal tube in the bronchus intermedius causes collapse of the right upper lobe and the entire left lung. Collapse of the left lung, especially the left lower lobe, due to an endotracheal tube (arrows) in the right main-stem bronchus that effectively blocks the passage of air into the left bronchial tree. Note the change in position of the calcified granuloma when the left lung collapses (arrow). The elevated right hemidiaphragm (2) is obliterated posteriorly by the airless right lower lobe, and the anterior third of the left hemidiaphragm (3) is obscured by the bottom of the heart. The overlapping shadows of the back of the heart (4), which lies in the left hemithorax, and the right hemidiaphragm simulate interlobar effusion. Develops in patients with asthma and hypersen- sitivity (allergic) bronchopulmonary aspergillosis. Chronic obstructive Segmental or subsegmental collapse (also Obstruction of small airways with the formation pulmonary disease evidence of underlying disease). Peribronchial inflammation may lead to small airway obstruction followed by collapse. Cystic fibrosis Lobar, segmental, or subsegmental collapse Small airway obstruction due to excessively superimposed on a coarse interstitial pattern. Most commonly because of tuberculosis (volume stricture Usually evidence of an alveolar or interstitial loss of the upper lobe). Fractured bronchus Lobar or segmental collapse with characteristic Result of severe thoracic trauma. The lymph Chronic process caused by quiescent granulo- node producing the compression may contain matous lymphadenitis (histoplasmosis, tuberculo- calcium. Hilar adenopathy is often cited as the cause of collapse, although the volume loss probably reflects the underlying pathologic process (eg, primary bronchogenic carcinoma, tuberculosis). To support this view, sarcoidosis is associated with profound hilar adenopathy yet rarely causes any volume loss. Radiation therapy Lobar or segmental collapse (often a peculiar Late scarring may produce a substantial loss of nonanatomic distribution of volume loss that volume superimposed on a characteristic inters- coincides with the radiation port). Broncholithiasis Lobar or segmental collapse associated with Results from erosion of a calcified lymph node into intrabronchial calcification. Eccentric calcification in the mass may indicate a bronchogenic car- cinoma growing around the histoplasmoma. Other granulomatous Central calcification that may be multiple or Tuberculosis, coccidioidomycosis. Eccentric (Fig C 19-3) calcification in the mass may indicate a broncho- genic carcinoma growing around the granuloma. Plasma cell granuloma Fine or coarse calcification in a parenchymal Common inflammatory pseudotumor of the lung (Fig C 19-4) nodule. Occasionally the process is aggressive and encases bronchi or invades mediastinal structures, chest wall, or diaphragm. Fungus ball Various patterns of calcification of the mycelial Scattered small nodules of calcification, a fine rim mass may occur. Develops in adults 1 or more years after pulmonary pneumonia chickenpox infection. The calcifications vary in size (Fig C 19-5) and number and predominate in the lower half of the lungs. Multiple tiny calcific shadows are scattered widely and uniformly throughout both lungs. This 42-year-old Fig C 19-6 asymptomatic man had had florid chickenpox with Calcified mucoid impaction in bronchial acute pneumonia 15 years earlier. Popcorn-ball calcification is pathognomonic (but (Fig C 19-7) occurs in less than 10%). Punctate calcifications are reported to occur in (Fig C 19-8) silicotic nodules in up to 20% of cases. Alveolar microlithiasis Widespread tiny, discrete, sand-like opacities of Tiny spherules of calcium phosphate in myriad (see Fig C 2-15) calcific density. Black pleura sign (caused by the contrast between the extreme density of the lung parenchyma on one side of the pleura and the ribs on the other). Manifestation of mitral stenosis (or other causes of elevated left atrial pressure). At up to 8 mm in size, usually much larger than the calcifications (up to 3 mm) of healed infectious diseases such as histoplasmosis or varicella.
The presence of an intermittent swelling suggests a pulsion diverticulum 75 mg triamterene overnight delivery blood pressure medication for cats, venous distention of congestive heart failure buy generic triamterene 75mg on-line pulse pressure of 53, a bronchial cyst cheap 75mg triamterene amex heart attack cafe menu, a stone of Wharton’s duct order triamterene 75mg on-line arteria cerebri media, and aneurysms. The presence of tremor or tachycardia would make one think of Graves’ disease and subacute thyroiditis. A radioactive iodine uptake and scan will help differentiate thyroid tumors and enlargements. Ultrasound and needle aspiration will be needed in differentiating cystic adenomas. A lymph node biopsy will be useful in 453 diagnosing sarcoidosis, lymphomas, and metastatic carcinoma. The presence of acute nightmares should make one think of the possibility of infectious disease, acute situational maladjustment, or a head injury. Chronic nightmares may be associated with drug or alcohol use, epilepsy, and neuroses or psychoses. Nightmares following trauma may be due to the acute anxiety associated with the trauma or actually to a head injury. Nightmares may result from complex partial seizures without tongue biting or incontinence. A urine drug screen will help rule out the possibility of drug-induced nightmares. If epilepsy is strongly suspected, a therapeutic trial of anticonvulsants may be necessary. If the workup is negative, referral to a psychiatrist or psychologist is in order. If there is daytime frequency, the differential diagnosis of polyuria should be considered (page 400). If this is above normal, the differential diagnosis of polyuria should be considered and additional workup can be found on page 400. Catheterization for residual urine will help determine if there is bladder neck obstruction. Structural abnormalities of the palate indicate cleft palate, congenital short soft palate, trauma, tuberculosis, syphilis, carcinoma, leprosy, and post-tonsillectomy scarring. Congenital abnormalities of the palate include cleft palate and congenital short soft palate. Acquired abnormalities of the palate include trauma, syphilis, tuberculosis, carcinoma, leprosy, and post-tonsillectomy scarring. The finding of paralysis of the soft palate may suggest myasthenia gravis, poliomyelitis, Guillain– Barré syndrome, pseudobulbar palsy, brain tumor, basilar artery insufficiency, and syphilitic meningitis. The presence of hypoactive reflexes would suggest poliomyelitis or Guillain–Barré syndrome. The presence of hyperactive reflexes or sensory findings would suggest pseudobulbar palsy, a brain tumor, basilar artery insufficiency, and syphilitic meningitis, among other conditions. It is best to consult an ear, nose, and throat specialist or a neurologic specialist before ordering expensive diagnostic tests. Pendular nystagmus without a fast or slow component suggests ocular nystagmus due to albinism, partial blindness, or other ocular disorders. Intermittent or fatigable nystagmus suggests otologic disorders, such as acoustic neuroma, Ménière’s disease, vestibular neuronitis, and acute labyrinthitis. The presence of nystagmus with tinnitus or deafness also suggests otologic disorders, such as acoustic neuroma, Ménière’s disease, or cholesteatoma. If there are long tract signs, multiple sclerosis and brain stem tumors must be considered. Nystagmus brought on by certain changes of position suggests benign positional vertigo. However, this also may be found in post-traumatic labyrinthitis and postconcussion syndrome. The presence of long tract signs suggests multiple sclerosis, basilar artery insufficiency, syringomyelia, and Friedreich’s ataxia. A spinal fluid analysis will help diagnose central nervous system lues and multiple sclerosis. The help of a neurologic specialist should be sought before ordering expensive diagnostic tests. Cisternography, tomography, and vertebral–basilar angiography are occasionally necessary to establish the diagnosis. If the patient recognizes that he or she has a ravenous appetite or eats more than is necessary, the possibility of an insulinoma or Fröhlich’s syndrome should be considered. The presence of centripetal obesity, especially with moon facies, should suggest Cushing’s syndrome. The presence of mental retardation should suggest Laurence–Moon–Bardet–Biedl syndrome. In male patients, one should consider Klinefelter’s syndrome, and in female patients, one should consider polycystic ovary. Many drugs may cause obesity, most notably the tricyclic antidepressants and corticosteroids. If an insulinoma is strongly suspected, plasma insulin, C-peptide, a 24- to 36-hour fast, a 5-hour glucose tolerance test, and tolbutamide tolerance test may be done. If Cushing’s syndrome is suspected, a 24-hour urine free cortisol and cortisol suppression test should be done. The presence of coma or disturbances of consciousness should suggest alcoholism, diabetic acidosis, uremia, and hepatic coma. The presence of a sweet odor to the breath should suggest diabetic acidosis, alcoholism, and maple syrup urine disease. The presence of an unpleasant or foul odor should suggest uremia, hepatic coma, anaerobic infections in the mouth or nasopharynx, and isovaleric aciduria. A culture of the mouth, gums, and nasopharynx may be necessary to diagnose anaerobic infections. If it is acute, strychnine poisoning, tetanus, and phenothiazine intoxication should be considered. If there is no recent wound infection, but a history of oral or intravenous drug use, tetanus, and strychnine poisoning are both possibilities. The presence of chronic or recurring opisthotonus should suggest epilepsy, Stiffman syndrome, and hysteria. The presence of incontinence or tongue biting in a chronic recurring form of opisthotonus should suggest epilepsy. If the opisthotonus is acute and there is a significant fever, one should consider meningitis. However, strychnine poisoning and tetanus may also induce fever in the later stages. A spinal fluid analysis, smear, and culture are indicated if meningitis is suspected. This symptom is the most characteristic of congestive heart failure, especially left ventricular failure.
The recti muscles which inert on to the pubic rami become widely separated from each other in the lower part of the abdomen buy discount triamterene 75 mg online blood pressure charts readings. In incomplete variety the pubic bones are united and the external genitalia are almost normal or there is epispadias generic triamterene 75mg heart attack jack look in my eyes. Due to pressure of the viscera behind it buy 75 mg triamterene amex blood pressure ranges for elderly, the posterior wall of the bladder protrudes through the defect cheap triamterene 75 mg hypertension occurs when. When this mucous membrane is gently pulled upwards, more pale wet trigone becomes visible. A line of demarcation becomes obvious between the protruding mucous membrane and the adjacent skin. When the exposed bladder wall is pushed behind with the fingers the firm edge beneath the mucocutane ous junction can be felt as the defect in the abdominal wall. Associated abnormalities — Other congenital anomalies are frequently associated with it. The femurs are rotated externally and the child waddles like a duck (waddling gait). Bilateral hemiae may be associated with undescended testes when sex differentiation becomes difficult. It may make the patient’s life miserable and it is difficult to control such infection. Metaplastic change may take place at the exposed mucous membrane of the urinary bladder and this may initiate formation of adenocarcinoma. Stricture at the site of anastomosis (uretero-sigmoidal), recurrent pyelonephritis and hyperchloraemic acidosis are the reasons of ultimate death of patients. Diversion of urine into an ileal conduit with excision of the bladder can be performed at 5 years of age. Recently attempts are being made to reconstruct the bladder and sphincter within first year of life. At first osteotomy of both iliac bones are made just lateral to the sacroiliac joints, the bladder is closed. Similarly urinary infection and stone formation and ultimately renal failure are also difficult to control. Various operations have been suggested for incontinence at bladder neck region, but overall success rate is limited. Normally the urachus is obliterated and is represented by a fibrous cord which is called median umbilical ligament and extends from the apex of the bladder to the umbilicus. Though this is congenital, yet this is only manifested in the adult or even old age. The reason is that contraction of the bladder starts at the apex of the organ and passes towards the base and ultimately to the neck As the urachus opens at the apex of the bladder, it is closed during contractions of the bladder and urine does not come out through the patent urachus. Urinary leakage through the umbilicus which reveals urinary fistula, becomes only evident when there is some urinary obstruction at the lower urinary tract e. If still the leak continues, the treatment is excision of the umbilicus with excision of the urachus down to the apex ofthe bladder with closure of the urinary bladder. The umbilical end ofthe urachus fails to obliterate giving rise to urachal sinus of the umbilicus. Sometimes the vesical end fails to obliterate, whereas the umbilical end obliterates normally. It represents an immobile swelling in the midline in the hypogastrium deep to the umbilicus. Sometimes adenocarcinoma may occur in a urachal cyst or in the patent vesical end of the urachus. So injuries to the bladder may be either extraperitoneal, which constitute 80% of bladder injuries or intraperitoneal which constitute 20% of all bladder injuries. About 15% of all pelvic fractures are associated with concomitant bladder or urethral injuries Intraperitoneal injuries are usually caused by a blow or kick or fall on to a fully distended bladder. There are other causes of injury to the bladder which include stab wounds and gun shot wounds. This causes extravasation of urine which has been discussed in detail in chapter 59 of The Prostate & Urethra’. Gradually infection may develop to cause deep pelvic abscess and severe pelvic inflammation from extravasation. When the bladder is full to its capacity, a direct blow to the lower abdomen may cause bladder disruption. Usually a linear laceration occurs at the dome of the bladder which will allow the urine to flow into the peritoneal cavity. If the urine is sterile, patient may not complain of any symptom for several days and diagnosis remains obscure If the urine is infected, immediate peritonitis and acute abdomen will develop. The diagnosis of pelvic fracture is easily made by lateral compression on the bony pelvis, which will evoke pain and crepitus at the fractured site. When this is associated with lower abdominal and suprapubic tenderness one may suspect extraperitoneal rupture of the bladder. The patient often tries to pass urine, when blood and even clots in the urine will come out. But catheterisation will be difficult or impossible in case of urethral injury with bloody discharge A plain X-ray demonstrates pelvic fracture. There may be haziness over the lower abdomen due to blood and urine extravasation. An excretory urography should always be performed to exclude kidney and ureteral injuries. About 120 ml of sterile isotonic saline is mixed with 60 ml of 35% Hypaque or Conray and this solution is introduced into the bladder and an X-ray is taken. This will demonstrate areas of extraperitoneal extravasation With intraperitoneal rupture, this examination will show free contrast medium within the abdomen. Cystoscopy is not very helpful as bleeding and clot obscure visualisation and prevent accurate diagnosis Intraperitoneal rupture — The peculiarity of this condition is that after the rupture, the patient often neither has any complaint, nor he feels the desire to pass urine. Sometimes patient complains of sudden, agonising pain in the hypogastrium with severe shock. Such injury to the bladder often occurs by direct blow to the full bladder in a drunk patient. Though the patient has not passed urine, yet the bladder is not distended as evident by percussion This is an important sign and should be remembered by the students. A plain X-ray in the erect position may show ground-glass appearance of the lower abdomen due to presence of urine in the peritoneal cavity. Instillation of radio-opaque solution into the bladder as mentioned in the extraperitoneal rupture often confirms the diagnosis. Before reaching the bladder, one may see pelvic haematoma and extravasation of urine.
Southern Prickly Ash. Triamterene.
- How does Southern Prickly Ash work?
- Are there safety concerns?
- Dosing considerations for Southern Prickly Ash.
- What is Southern Prickly Ash?
- Are there any interactions with medications?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96117